

Addiction Recovery Statistics: Recovery Rates, Relapse & Rehab Data
If you or someone you love is wondering how many people actually recover from addiction, you are not alone in searching for a clear answer.
About 9.1% of U.S. adults, roughly 22 million people, report having resolved a substance problem, and 40% to 60% of people in specialty care remain abstinent or avoid heavy use at the one year mark.
This article breaks down what addiction recovery statistics really show, who recovers, what percent of addicts relapse, and which factors shift the odds.
What Addiction Recovery Statistics Tell Us?
The honest truth is that no single number captures addiction recovery rates. The figure you see depends on how “recovery” is defined, which substance is involved, how long researchers followed people, and whether the study counted total abstinence or stable, low risk use.
Large national surveys like the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) sort people into distinct categories: abstinent recovery, nonabstinent recovery, partial remission, and more.
NESARC researchers required nonabstinent recovery to meet strict criteria, including no abuse or dependence symptoms and drinking within low risk limits set by the NIAAA. That means “recovery” in the data is not just wishful thinking. It is measured against clear clinical thresholds.
How many people recover from addiction?
The National Recovery Study found that about one in eleven U.S. adults have resolved a significant alcohol or other drug problem.
Among those 22 million people, more than half do not call themselves “in recovery.” Many say they resolved the problem with little or no formal help. Mutual help groups like AA were the most common support among those who did seek outside help.
These numbers reflect lifetime problem resolution, not a single treatment episode. They include people across a wide range of severity. Someone who struggled with heavy drinking for a few years and stopped on their own sits alongside someone who completed multiple rounds of rehab. Both count.
Abstinent vs. nonabstinent recovery
Recovery does not always mean total abstinence. For alcohol, nonabstinent remission, meaning symptom free use within safe limits, is more common.
For drug problems, especially opioids, abstinence is the more typical path. NESARC data formalized by Dawson and colleagues show that both endpoints can be durable and clinically meaningful when properly measured.
This distinction matters because addiction recovery rates look different depending on which definition a study uses. Including nonabstinent remission raises the measured rate, especially for alcohol. Excluding it paints a narrower picture.
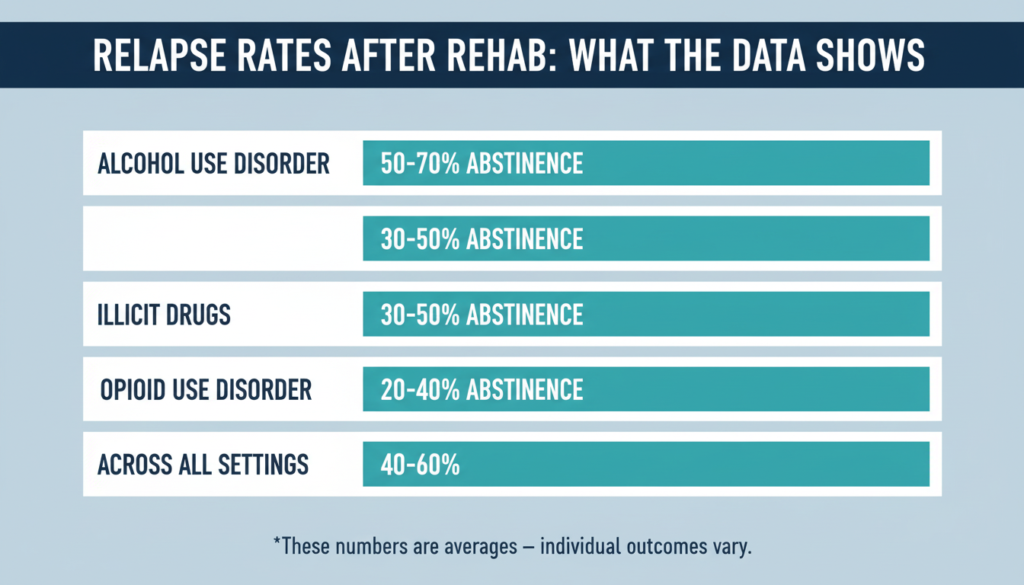
Addiction Recovery Rates by Substance and Setting
Alcohol use disorder
Across intensive outpatient and residential programs, about 40% to 60% of people with alcohol use disorder are abstinent or not drinking heavily at the six to twelve month mark.
One hospital cohort showed an early advantage for inpatient care: roughly 25% of inpatients returned to heavy drinking by two months compared with about 50% in outpatient care.
By six months, both groups converged near 50%, showing that the initial setting matters less over time than what happens after discharge.
Long term data tell a more encouraging story. Among people with alcohol use disorder who attended AA for 27 or more weeks in their first year, outcomes were significantly better 16 years later.
Part of formal treatment’s long term benefit appeared to flow through sustained AA involvement, suggesting that ongoing connection is a powerful driver of lasting change.
Illicit drugs and polysubstance use
In a prospective study of inpatients treated for illicit drug use, about 37% relapsed within 90 days of discharge. Younger adults and those with psychiatric conditions faced higher risk.
Notably, treatment at longer term clinics (over six months) was linked to lower relapse regardless of how long any individual stayed, pointing to the clinic environment itself as a protective factor.
Opioid use disorder
For opioid use disorder, the most important recovery statistic is not an abstinence percentage. It is survival. A BMJ meta analysis found that all cause mortality during methadone treatment was 11.3 per 1,000 person years compared with 36.1 out of treatment.
For buprenorphine, the rate was 4.3 in treatment versus 9.5 out of treatment. Risk spiked sharply in the first four weeks after stopping medication, then declined.
Veterans Health Administration data echo this pattern. Days off buprenorphine carried a 4.33 fold higher risk of suicide or overdose death compared with days on treatment, with the highest danger 8 to 14 days after stopping.
A synthesis of 28 longitudinal OUD cohorts shows that multiple treatments and relapses are common before sustained remission. The risk of relapse drops substantially after about five years of continuous remission, reinforcing the chronic care model.
What Percent of Addicts Relapse After Rehab?
There is no universal relapse rate. But credible ranges, broken down by substance and timeframe, give a realistic picture.
- Alcohol use disorder, 6 to 12 months post treatment: About 40% to 60% remain abstinent or avoid heavy drinking. Early relapse risk is higher and sensitive to depression, low self efficacy, and lack of continuing care.
- Illicit drugs, first 3 months post inpatient: Roughly 30% to 40% relapse, with younger age and psychiatric comorbidity raising risk. Longer term clinic environments reduce this figure.
- Opioid use disorder: Multiple treatment episodes and relapses are typical before sustained remission. Medication retention is the strongest predictor of survival and stability. Most Medicaid patients on either extended release naltrexone or buprenorphine discontinue within six months.
- Across settings at 6 to 12 months: Inpatient and intensive outpatient programs produce broadly similar outcomes (50% to 70% abstinent) when severity and retention are accounted for. Early advantages for residential care tend to fade by six months.
These numbers are not destiny. They describe averages across populations, and individual outcomes shift based on what happens after the initial treatment episode.
Why So Few People Get Evidence Based Care?
The 2023 National Survey on Drug Use and Health paints a stark picture of the gap between need and treatment.
| Indicator (ages 12 and older) | Estimate |
|---|---|
| Received any substance use treatment in the past year | 4.5% |
| Received outpatient treatment | 3.5% |
| Outpatient care delivered outside general medical settings | 82.6% |
| Adults with co occurring SUD and mental illness receiving both treatments | 18.6% |
| Adults with co occurring SUD and mental illness receiving neither | 37.6% |
| People with OUD receiving medication for OUD | 18% |
Only 18% of people with opioid use disorder received medication in 2023. That single figure represents one of the largest missed opportunities in American healthcare.
Medications like methadone and buprenorphine are cost effective, reduce infectious disease transmission, and save lives. Yet regulatory barriers, fragmented care, and uneven state policies keep them out of reach for most people who need them.
Meanwhile, 37.6% of adults dealing with both a substance use disorder and a mental illness received no treatment for either condition. Addiction care remains largely separated from general medical and mental health services, and that separation costs lives.
What Predicts Relapse and What Prevents It?
Decades of research point to a consistent set of factors that raise or lower relapse risk.
Low self efficacy and poor coping skills are among the strongest proximal predictors. The Alcohol Abstinence Self Efficacy Scale (AASE) shows excellent reliability across major clinical trials and can be tracked over time to flag rising risk.
Interestingly, early behavioral wins, like confirmed abstinence through contingency management, appear to build self efficacy in a positive feedback loop. Reducing heavy drinking increases confidence in staying sober, which in turn supports continued abstinence.
Depressive symptoms consistently predict relapse in alcohol use disorder and elevate risk after inpatient care for other substances.
Depression erodes coping and creates the negative emotional states that classic relapse models identify as high risk triggers. Treating depression alongside addiction is not optional. It is essential.
Sustained mutual help participation is one of the most reliable long term protective factors. The dose matters: 27 or more weeks of AA in the first year predicted better outcomes 16 years later.
A national longitudinal study during the pandemic found that alcohol outcomes improved regardless of whether people attended mutual help groups online, in person, or both. Engagement itself, not the format, drove improvement.
Structured continuing care extends the treatment window. Telephone based monitoring and counseling platforms that run 12 to 18 months after intensive outpatient care help people stay connected, practice coping skills, and catch warning signs early.
Routine AASE tracking gives clinicians a measurement based tool to guide adaptive care rather than waiting for a crisis.
Recovery housing likely reduces early relapse by providing a stable, sober environment during the highest risk months. A 2025 systematic review found only three randomized trials on recovery housing, with the longest average follow up at 18 months.
The evidence is promising but thin, and updated research with economic evaluations is urgently needed.
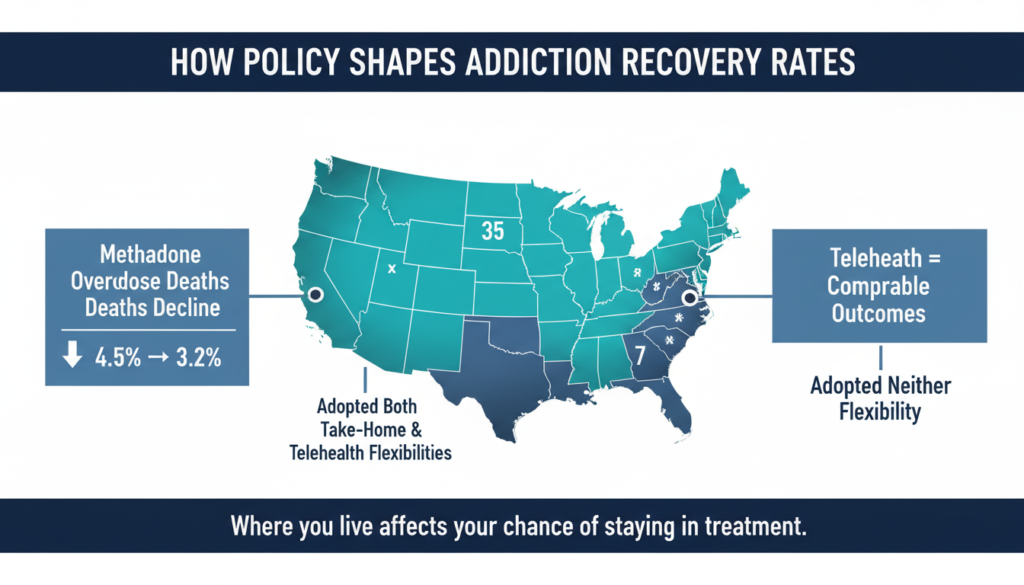
How Policy Shapes Addiction Recovery Rates?
Recovery does not happen in a vacuum. Policy decisions about medication access, telehealth, and harm reduction directly affect how many people recover from addiction.
During the pandemic, SAMHSA allowed up to 28 days of take home methadone for stable patients. Multiple studies found this flexibility did not increase methadone involved overdose deaths.
The share of overdose deaths involving methadone actually declined from 4.5% in January 2019 to 3.2% by August 2021. Expanded take homes were linked to better engagement, higher patient satisfaction, and few diversion incidents.
Yet state uptake varied widely. Thirty five jurisdictions adopted both take home and telehealth flexibilities. Seven adopted neither. That patchwork means a person’s chance of staying in treatment, and staying alive, partly depends on geography.
Telehealth buprenorphine showed comparable outcomes to in person care and improved retention in some groups. No increase in buprenorphine involved overdose deaths appeared among Medicare beneficiaries receiving telehealth prescriptions.
These findings argue strongly for making flexible, low barrier medication access permanent.
Why These Numbers Matter?
Addiction recovery statistics are not abstract. They represent real people making real attempts to rebuild their lives. When we look at the data honestly, a few things become clear.
Recovery is more common than most people think. Roughly one in eleven American adults have resolved a serious substance problem. Many did it quietly, without formal treatment, and without ever calling themselves “in recovery.”
Relapse is common but not inevitable. The first three to six months after treatment carry the highest risk, and that risk responds to specific, evidence based actions: staying in care longer, treating depression, attending mutual help groups regularly, tracking self efficacy, and living in a stable environment.
For opioid use disorder, the gap between what works and what people actually receive is enormous. Only 18% of those with OUD got medication in 2023. Closing that gap is the single most powerful lever to raise real world recovery rates and prevent deaths.
And how we define and measure recovery shapes the numbers we see. Including nonabstinent remission for alcohol, using prospective rather than only retrospective designs, and accounting for people who drop out of studies all change the picture.
As the National Academies have cautioned, recovery rate headlines must disclose definitions, timeframes, and methods to mean anything at all.
The bottom line: recovery from addiction is achievable, measurable, and improvable. The question is not whether people can recover. It is whether our systems give them a fair chance.
If you or someone you care about is ready to take the next step, reaching out for professional support can make a real difference. Learn more about Mosaic Behavioral Health Center’s available programs and services.