

How Does PHP vs IOP Affect Your Level of Mental Health Care?
Choosing the wrong level of care can slow your recovery or leave you without enough support when you need it most.
PHP vs IOP is not just a scheduling question — it is a clinical decision that shapes how much structure, monitoring, and therapeutic contact you receive each day.
This article breaks down how each program works, who each one fits best, and how to think through the choice for depression, addiction, or broader mental health needs.
How PHP vs IOP Shapes Your Mental Health Treatment?
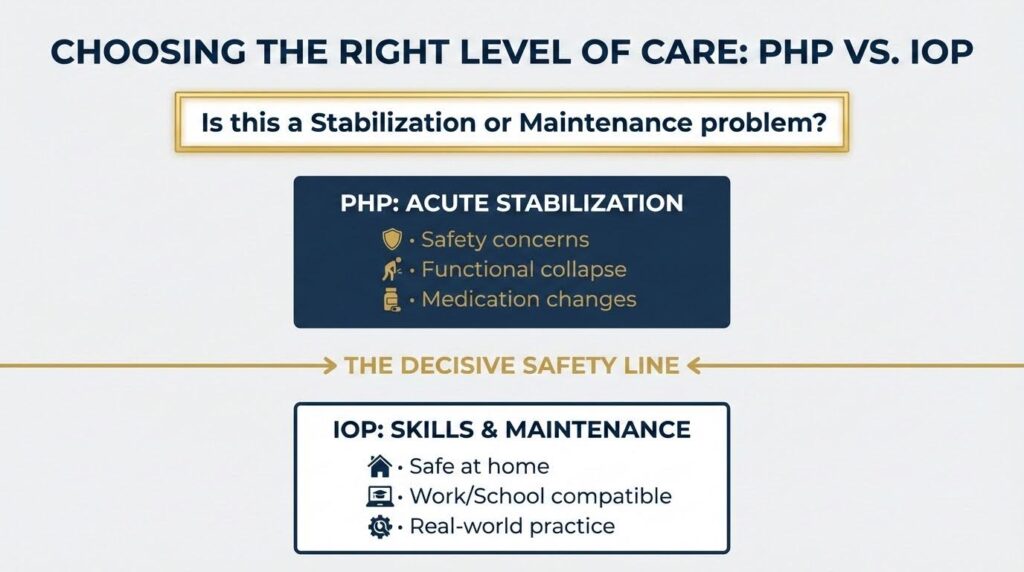
The clearest way to understand the difference: PHP organizes your day around treatment, while IOP fits treatment around your day. That single distinction drives nearly every other difference between the two programs.
A partial hospitalization program typically runs five days a week for five to six hours each day, adding up to roughly 20 to 30 hours of structured care per week.
An intensive outpatient program usually meets three to five days a week for about three hours per session, totaling nine to fifteen hours weekly.
Both allow you to sleep at home. Neither requires overnight admission. But the gap in intensity between them is significant, and placing someone at the wrong level can mean the difference between stabilizing and sliding backward.
The ASAM Criteria, the most widely used placement framework in addiction treatment, formally labels PHP as Level 2.5 and IOP as Level 2.1. That numbering reflects a real clinical difference, not just an administrative one.
What Each Program Actually Looks Like Day to Day?
Inside a Partial Hospitalization Program
A typical PHP day might start with a morning check-in group, move into psychoeducation, then individual therapy, then a skills group using cognitive behavioral therapy or dialectical behavior therapy, and close with medication management or discharge planning.
Psychiatric oversight happens daily or near-daily. The structure is intentional: it is designed to hold you steady when your own routines cannot.
PHP is most often used in three situations. First, as a step-down after inpatient psychiatric care or residential addiction treatment, when you are no longer in crisis but still too fragile for less intensive support.
Second, as a way to avoid hospitalization altogether when symptoms are serious but you can remain safe at home overnight. Third, as a step-up when standard outpatient therapy or IOP is no longer enough.
One peer-reviewed study of a virtual PHP found that patients in the telehealth format had a hospitalization rate of 8.9 percent, compared to 16.5 percent for in-person PHP patients, and attendance was higher in the virtual group as well.
That finding matters because it shows that PHP-level care can prevent hospitalization when delivered well, even remotely.
Inside an Intensive Outpatient Program
IOP sessions typically run in the evening or morning, making it possible to keep working, attend school, or care for family members while still receiving structured treatment.
A session might include a check-in, a process group, a skills group focused on relapse prevention or emotional regulation, and a brief wrap-up with homework.
The defining feature of IOP is real-world application. You attend treatment, then go back into your life and practice what you learned. That is a strength when you are stable enough to handle it. It becomes a risk when you are not.
Intensive outpatient programs work best as a step-down from PHP or residential care, or as a step-up from weekly outpatient therapy that is no longer holding.
They assume you can stay safe between sessions and that your home environment is supportive enough to carry some of the therapeutic load.
Key Differences at a Glance
| Dimension | PHP | IOP |
|---|---|---|
| Typical weekly hours | 20 to 30 hours | 9 to 15 hours |
| Days per week | 5 to 7 | 3 to 5 |
| Psychiatric monitoring | Daily or near-daily | Less frequent, as needed |
| Primary clinical goal | Stabilization | Skill application and maintenance |
| Work or school compatibility | Often difficult | Usually feasible |
| ASAM level (addiction) | 2.5 | 2.1 |
| Best role in care pathway | Post-inpatient step-down or hospitalization diversion | Step-down from PHP or step-up from outpatient |
PHP vs IOP for Depression: How to Tell Which Fits?
Depression does not automatically point to one level of care. What matters is how severe the symptoms are, whether safety is a concern, and how much the depression is disrupting daily functioning.
PHP is usually the better fit for depression when:
- Symptoms are severe enough to make basic routines feel impossible
- There is recent suicidal ideation, self-harm concern, or a recent psychiatric hospitalization
- Medications have just been changed and need close monitoring
- Co-occurring conditions like anxiety, trauma, or substance use are making things more unstable
- Standard outpatient therapy or IOP has already failed to hold the person steady
IOP is usually the better fit for depression when symptoms are real and impairing but the person can stay safe at home, maintain some responsibilities, and benefit from structured therapy several times a week without needing daily clinical oversight.
A useful shorthand: if depression is a stabilization problem, PHP is likely the right answer. If it is a maintenance-and-application problem, IOP is likely enough.
One source focused specifically on PHP vs IOP for depression puts it plainly: choose PHP if daily functioning feels overwhelming or medication management and all-day structure are needed, and choose IOP when symptoms are serious but compatible with home living and skill-based treatment.
Safety is the decisive line. When depressive symptoms involve suicidal thinking, self-harm, or severe functional collapse, the risk of undertreatment is greater than the risk of overtreatment.
Placing someone in IOP when they need PHP because IOP is easier to schedule is one of the most common and consequential mismatches in behavioral health care.
IOP vs PHP for Addiction Treatment
For substance use disorders, the same core logic applies, but a few addiction-specific factors shift the calculation.
PHP is generally the better choice when:
- The person has just completed detox or inpatient rehab and is newly sober but unstable
- Relapse risk is high and cravings feel unmanageable in ordinary life
- There are active co-occurring psychiatric symptoms
- Previous attempts at IOP or outpatient treatment have ended in relapse
IOP is generally the better choice when:
- The person is medically stable and has a supportive home environment
- The goal is relapse prevention and accountability rather than daily stabilization
- Work, school, or caregiving responsibilities need to be maintained
- The person is stepping down from PHP or residential care and is ready to practice recovery in real life
One important insight from the addiction literature is that IOP may actually produce stronger long-term recovery habits than inpatient care for certain patients, because it allows people to identify and manage triggers in their real environment rather than a protected setting.
But that advantage only applies when the person is stable enough to survive that exposure. If they are not, home exposure becomes a relapse hazard rather than a therapeutic benefit.
The ASAM Criteria framework evaluates six dimensions to guide placement decisions: withdrawal potential, biomedical conditions, emotional and behavioral conditions, readiness to change, relapse potential, and the recovery environment.
That last dimension, the recovery and living environment, is one of the most overlooked. Someone with a chaotic or trigger-heavy home may need PHP or even residential care even if their symptom severity alone might suggest IOP.
The Role of Telehealth in PHP and IOP Access
Telehealth has changed the practical calculus for both programs, especially for people in rural areas or those facing transportation barriers.
The virtual PHP study mentioned earlier found that removing transportation as a barrier actually improved attendance and reduced hospitalization rates.
That finding has a direct implication: if a person clinically needs PHP but cannot access it in person, virtual PHP delivery may be a viable and effective option rather than defaulting to a lower level of care.
IOP adapts more easily to telehealth because of its shorter session blocks and lower need for daily medical monitoring. But the evidence suggests that PHP can also be delivered virtually without sacrificing outcomes when the program is well-structured.
As of January 2026, Medicare telehealth rules no longer require patients to be in a rural area to receive mental health services via telehealth from home, which expands access meaningfully for behavioral health programs at both levels.
PHP and IOP as a Sequence, Not a Competition
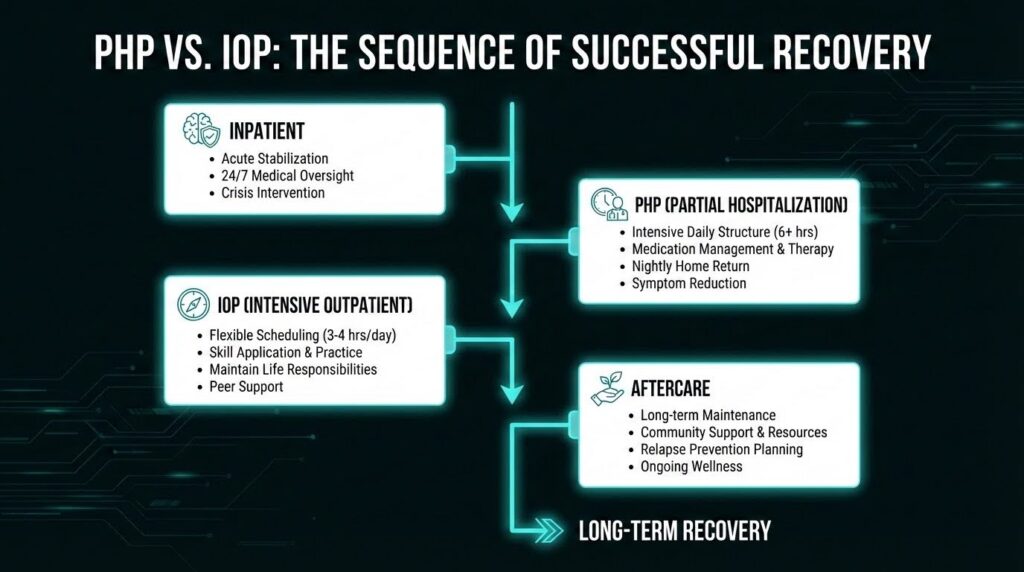
One of the strongest themes across the research is that PHP and IOP work best when treated as linked stages rather than competing options. The most common and effective pathway looks like this:
Detox or inpatient care leads to PHP for stabilization, which then steps down to IOP for continued structured recovery, which eventually transitions to standard outpatient therapy and aftercare.
SAMHSA’s 2025 National Behavioral Health Crisis Care Guidance reinforces this systems view, emphasizing coordinated continuums where people can move between levels of care based on need, with no wrong door for access and clear accountability for transitions.
The period immediately after leaving PHP or IOP carries its own risks. External stressors return, accountability drops, and the skills learned in treatment face their first real test.
Building the next step into the plan before discharge, whether that is IOP after PHP or outpatient therapy after IOP, is not optional. It is part of what makes the treatment work.
A Practical Decision Rule
If you are trying to decide between PHP and IOP for yourself or someone you care about, two questions cut through most of the complexity:
Does this person need treatment to organize and stabilize their day? If yes, PHP is likely the right level.
Can this person organize their day independently but still needs frequent, structured clinical support? If yes, IOP is likely enough.
The home environment matters as much as symptom severity. A stable, supportive living situation makes IOP more viable. An unstable, chaotic, or trigger-heavy environment pushes the need toward PHP or higher, regardless of how the clinical picture looks on paper.
And if access is the barrier rather than clinical need, it is worth asking whether a telehealth PHP or IOP option exists before settling for a lower level of care than the situation calls for.
Why Getting the Right Level of Care Matters?
Poor level-of-care matching creates two real problems. Undertreatment, placing someone in IOP when they need PHP, can lead to deterioration, relapse, or hospitalization.
Overtreatment, placing someone in PHP when IOP would serve them better, creates unnecessary burden, disrupts work and caregiving, and can reduce adherence over time.
The goal is not the most intensive program or the most convenient one. It is the one that matches where the person actually is, right now, with a clear plan for what comes next.
If you are ready to talk through which level of care fits your situation, reach out to our team at Mosaic to start the conversation.