7 Coping Skills for Addiction That Support Lasting Recovery
Coping skills for addiction are the practical strategies people use to manage cravings, stress, and triggers without returning to substance use.
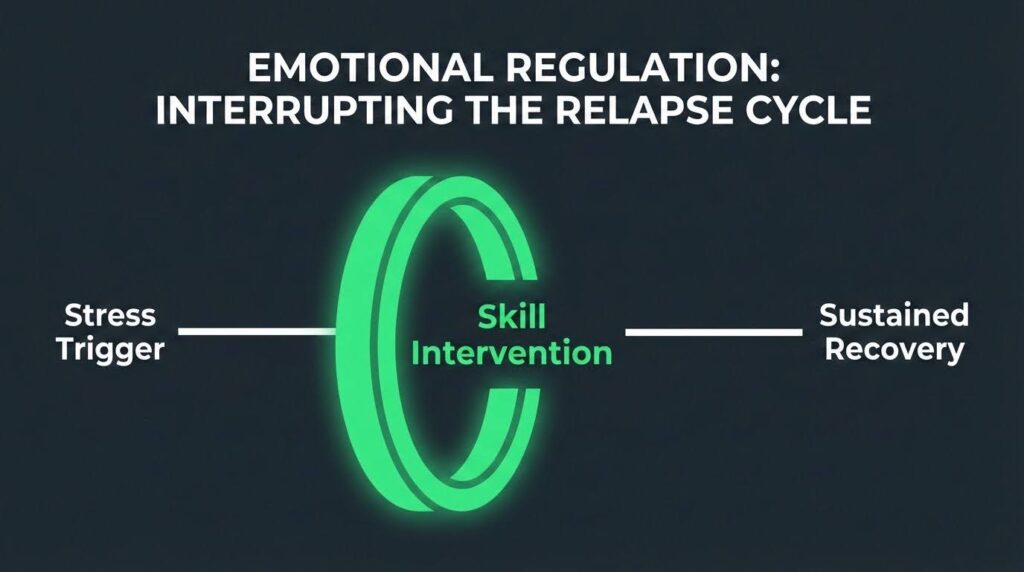
Research shows that relapse is rarely a sudden event; it typically unfolds across emotional, cognitive, and behavioral stages, which means the right skills, applied early, can interrupt the process before it escalates.
This article walks through seven of the most evidence-supported coping skills for addiction recovery and explains how each one works in real life.
Coping Skills for Addiction: Why They Matter?
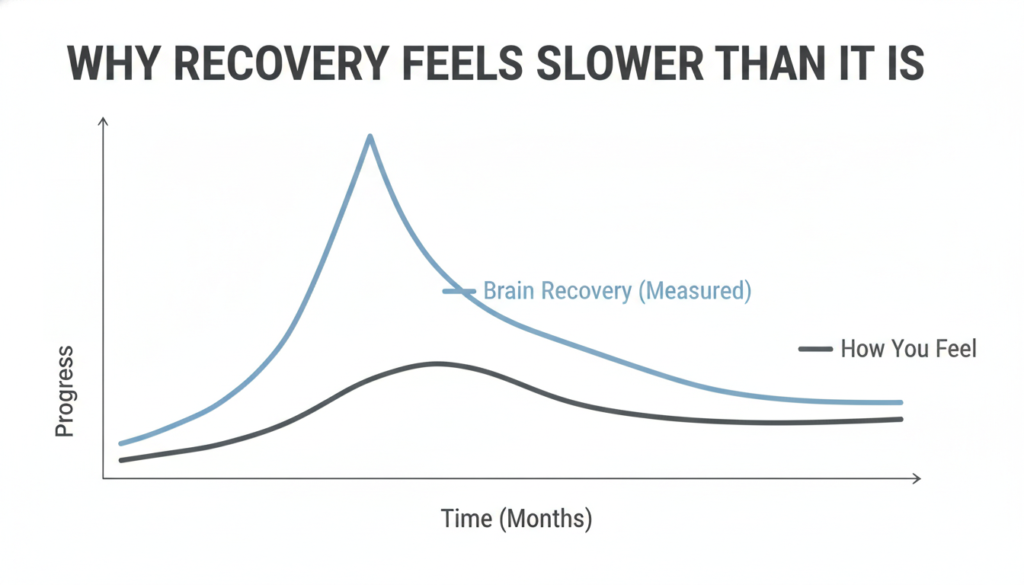
Many people assume that stopping substance use is the hardest part of recovery. In practice, learning to live without substances as a coping tool is often the longer challenge.
Addiction frequently becomes a person’s main method for managing stress, loneliness, shame, boredom, and emotional pain. When substances are removed, those underlying pressures remain.
Relapse prevention research describes recovery as “creating a new life where it is easier to not use.” That framing matters because it shifts the focus from white-knuckling through cravings to building a daily life that supports sobriety. Coping skills are the tools that make that new life possible.
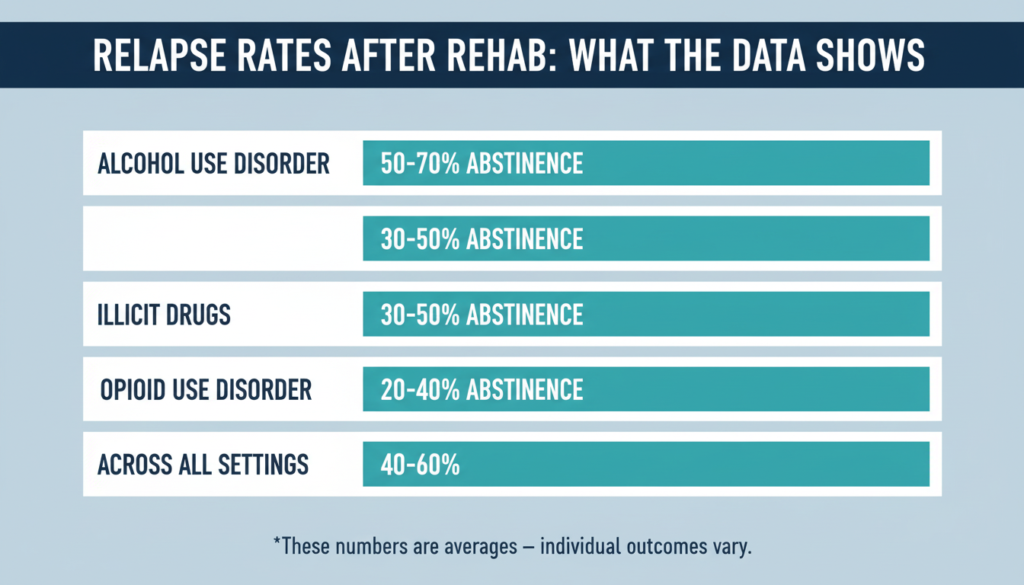
Relapse rates for substance use disorders are commonly estimated in the 40% to 60% range, comparable to other chronic health conditions.
That figure is not a reason for pessimism. It is a reason to take coping seriously as an ongoing practice rather than a one-time lesson learned in treatment.
1. Recognize Your Triggers Early
The single most important coping skill for addiction recovery is learning to spot warning signs before a craving peaks.
Relapse prevention models describe a predictable sequence: a high-risk situation arises, and if the person has no effective coping response ready, self-confidence drops and the chance of relapse rises sharply.
Triggers fall into two broad categories:
- Internal triggers include stress, anger, loneliness, shame, boredom, fatigue, and trauma-related feelings.
- External triggers include people tied to past use, places where substances were available, conflict situations, celebrations, and unstructured time.
A practical self-monitoring tool used across many recovery programs is the HALT check. Before acting on an urge, pause and ask: Am I Hungry, Angry, Lonely, or Tired?
The VA Whole Health guidance on reducing relapse risk presents HALT as a reminder that basic unmet needs can quietly raise vulnerability long before a conscious craving appears.
Keeping a daily log of moods, cravings, sleep quality, and social contact helps you spot patterns over time. When you know your personal trigger map, you can respond earlier and more deliberately.
2. Use Cognitive-Behavioral Coping Skills for Addiction
Cognitive-behavioral therapy is one of the most studied approaches in addiction treatment. It works by increasing the gap between a trigger and a response.
Instead of moving automatically from “I feel stressed” to “I need a drink,” a person learns to notice the thought, question it, and choose a different action.
Common thoughts that drive relapse include:
- “I can’t handle this sober.”
- “One time won’t matter.”
- “I’ve already messed up today, so it doesn’t matter.”
- “I deserve a reward.”
StatPearls addiction relapse prevention identifies cognitive-behavioral approaches among the most common and effective relapse prevention strategies.
The skill is not to suppress the thought but to examine it. Ask: Is this thought accurate? What is the likely outcome if I act on it? What have I done before when I felt this way?
Coping cards, written in advance, can help. A card might say: “This craving will pass in 20 to 30 minutes. Call someone. Change location. Review what I have to lose.” Having the response written down means you do not have to generate it under pressure.
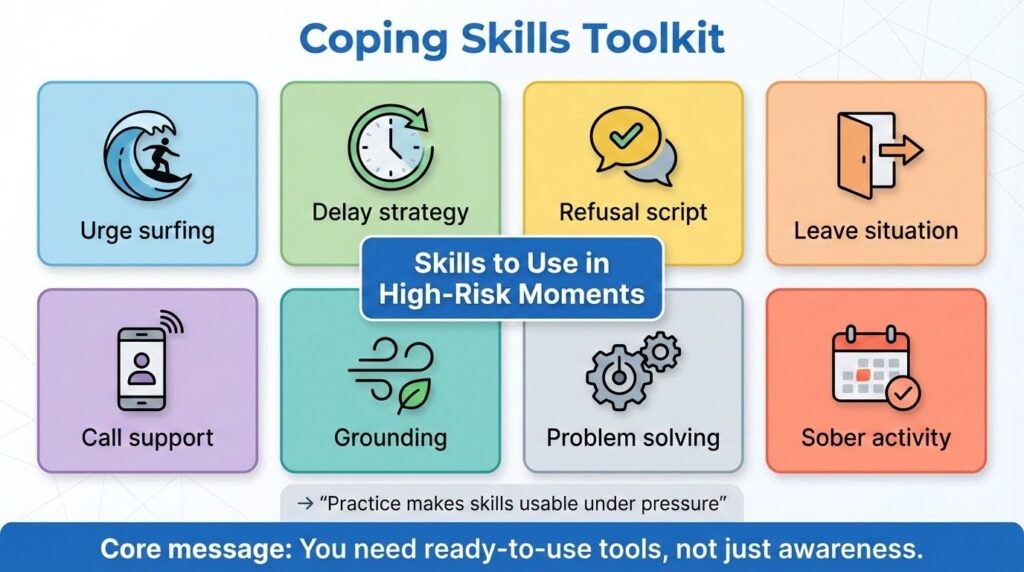
3. Manage Cravings Actively and Quickly
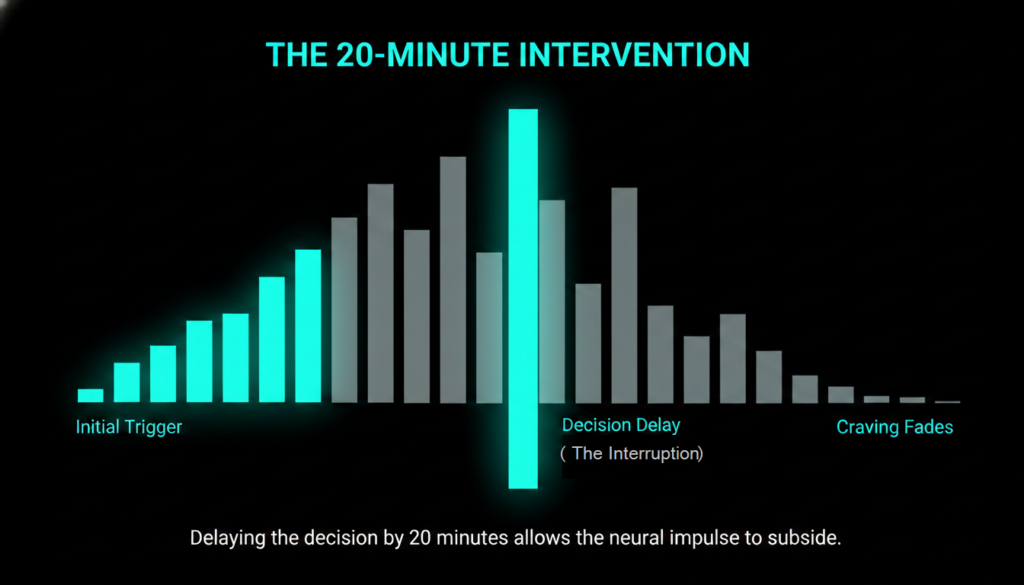
Cravings are not commands. They are temporary waves of discomfort that rise, peak, and fall. One of the most useful coping skills for drug addiction and alcohol recovery is learning to ride that wave rather than fight it or give in to it.
Urge surfing, a technique developed within mindfulness-based relapse prevention, teaches people to observe a craving with curiosity rather than alarm.
Notice where you feel it in your body. Rate its intensity from one to ten. Watch whether it rises or falls over the next few minutes. Most cravings peak and begin to ease within 20 to 30 minutes if you do not feed them.
Other craving-management steps that work well together:
- Leave the environment immediately if possible.
- Call or text a support person before the craving reaches its peak.
- Use slow, controlled breathing to lower physical arousal.
- Delay any decision by at least 20 minutes.
- Review your written relapse-prevention plan.
The key principle across all of these is to respond early. Waiting until a craving is at full intensity before acting makes every other skill harder to use.
4. Build a Structured Daily Routine
A structured daily routine may be the single most underappreciated coping skill in addiction recovery.
Research on habits and routines in early recovery found that consistent practices such as writing, prayer, and regular meeting attendance helped people in recovery structure their time, build social support, and maintain self-care. Participants specifically identified these routines as protective against relapse.
Routine matters for several practical reasons. It reduces idle time, which is a common trigger. It lowers decision fatigue by making recovery-supporting behaviors automatic rather than effortful.
It stabilizes sleep and meals, which directly affect mood and impulse control. And it creates a predictable framework within which other coping skills can be practiced.
A basic recovery routine might include:
- A consistent wake and sleep time
- Regular meals
- A daily self-check or HALT scan
- Scheduled therapy, meetings, or support contact
- Physical movement of some kind
- An evening wind-down with reflection or journaling
Routine is also the delivery system for every other coping skill. Sleep hygiene requires routine. Meeting attendance requires routine.
Medication adherence requires routine. When life becomes chaotic, coping skills are the first thing to slip.
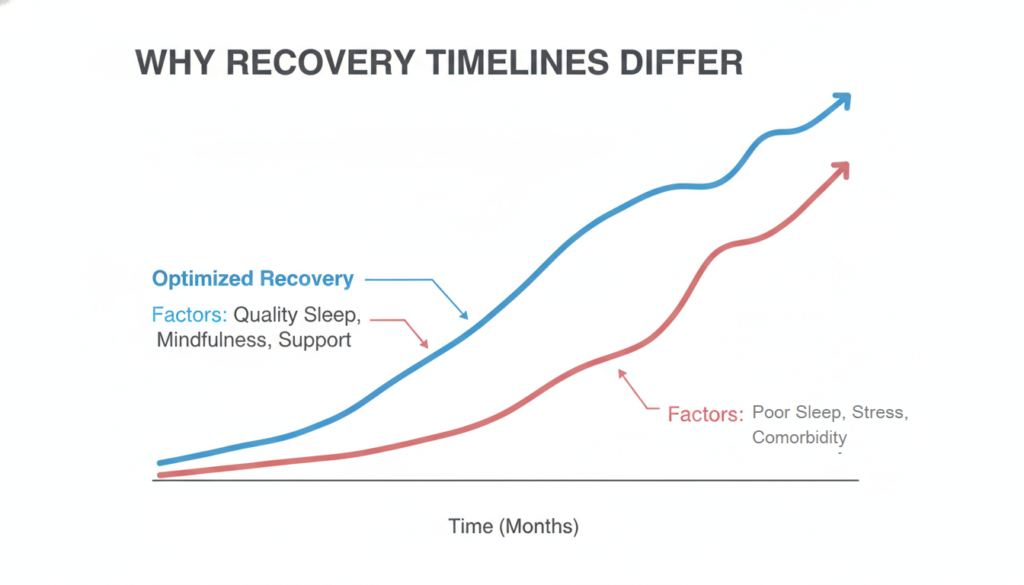
5. Prioritize Self-Care, Especially Sleep
Self-care is not a lifestyle preference in addiction recovery. It is a relapse-prevention strategy. The five rules of recovery described in foundational relapse prevention literature place self-care alongside honesty, help-seeking, and cognitive change as a core recovery principle.
Sleep deserves special attention. Poor sleep raises irritability, weakens impulse control, increases craving sensitivity, and reduces the effectiveness of every other coping skill.
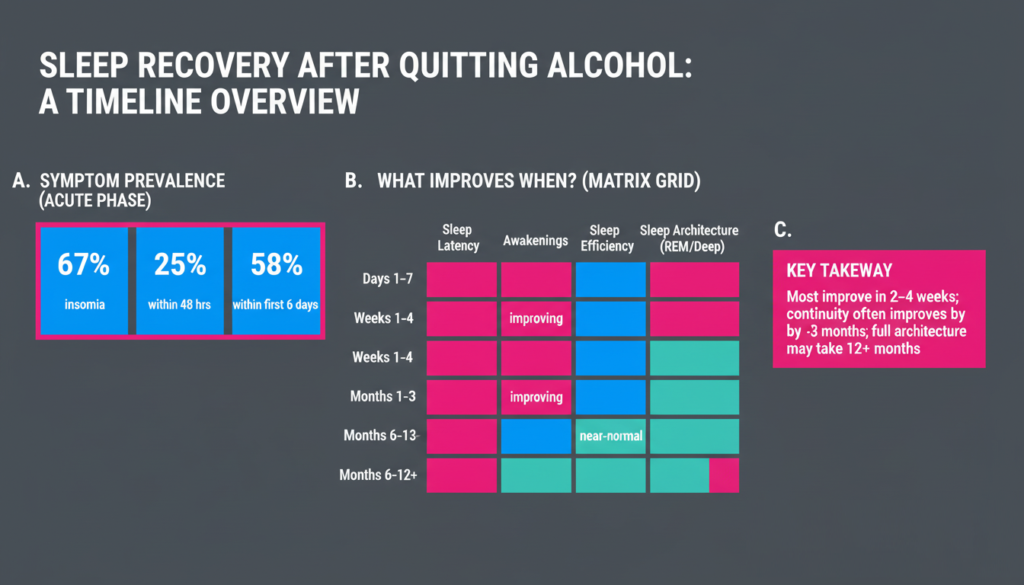
Research on long-term alcohol remission found that neurocognitive and physiological issues including sleep disruption continued to predict relapse risk well beyond the first year of recovery. Sleep problems are not just an early detox concern.
Nutrition and regular meals matter too. Stable blood sugar supports mood regulation and reduces the irritability that can quietly push a person toward high-risk thinking. Exercise, even moderate daily movement, helps with stress regulation, sleep quality, and structured time use.
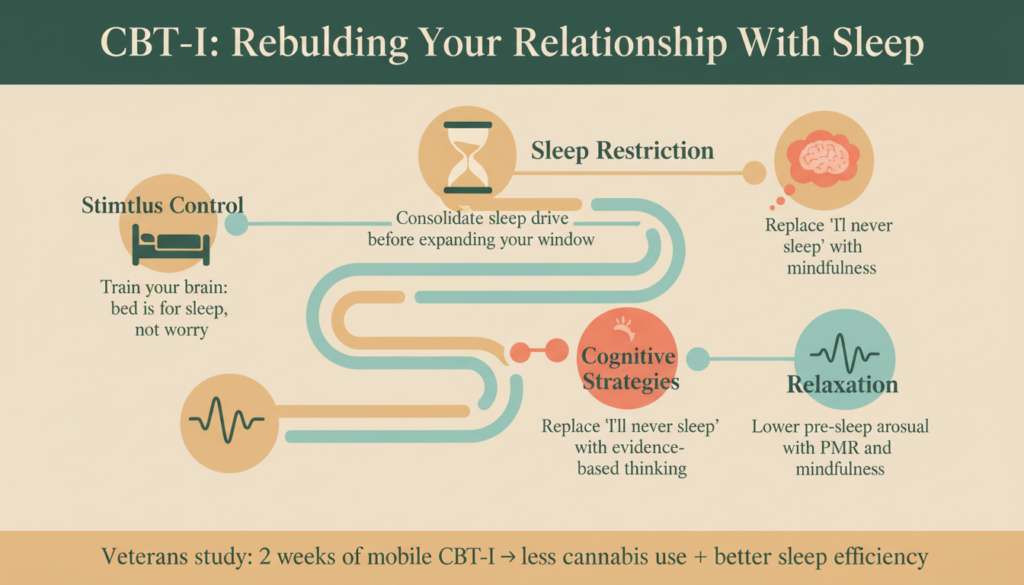
Mind-body relaxation, including paced breathing and progressive muscle relaxation, is identified in relapse prevention literature as one of the main tools for reducing physiological arousal during high-risk moments.
These practices are most useful when they are already part of a daily routine rather than something you try for the first time during a crisis.
6. Use Social Support as an Active Coping Skill
Social support is sometimes treated as a background condition of recovery rather than a coping skill in its own right. The evidence suggests that framing is wrong.
Actively using support is a behavior that requires honesty, initiative, and willingness to be known. It is one of the most protective things a person in recovery can do.
The VA Whole Health guidance states clearly that meeting attendance, active engagement, and having a sponsor are among the strongest predictors of abstinence over time.
A qualitative meta-synthesis on recovery coping found that self-awareness and personal responsibility, including reaching out for help, were central to overcoming recovery challenges.
Specific support-based coping behaviors include:
- Calling a sponsor or peer before acting on an urge, not after
- Attending a meeting the same day a major trigger occurs
- Telling someone you trust about warning signs you have noticed
- Participating in a recovery community, whether in person or online
- Keeping a list of emergency contacts and using it
Relapse tends to happen in secrecy and isolation. The more connected a person stays, the harder it is for the gradual drift toward relapse to go unnoticed.
7. Maintain Vigilance and Continuing Care Over Time
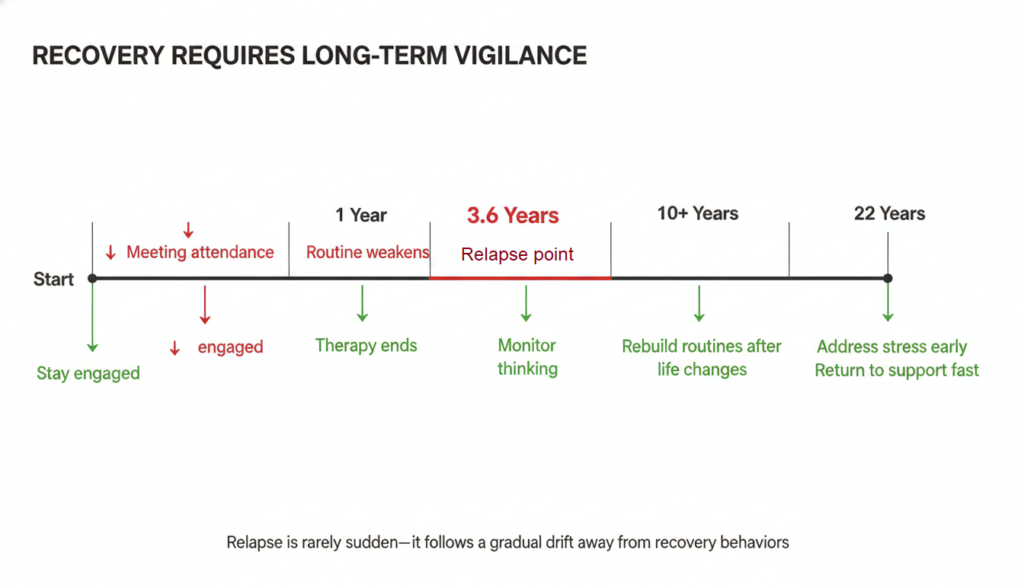
One of the most important findings in recent addiction research concerns long-term recovery. Among people with sustained alcohol remission who eventually relapsed, one of the strongest preceding changes was a reduced focus on recovery.
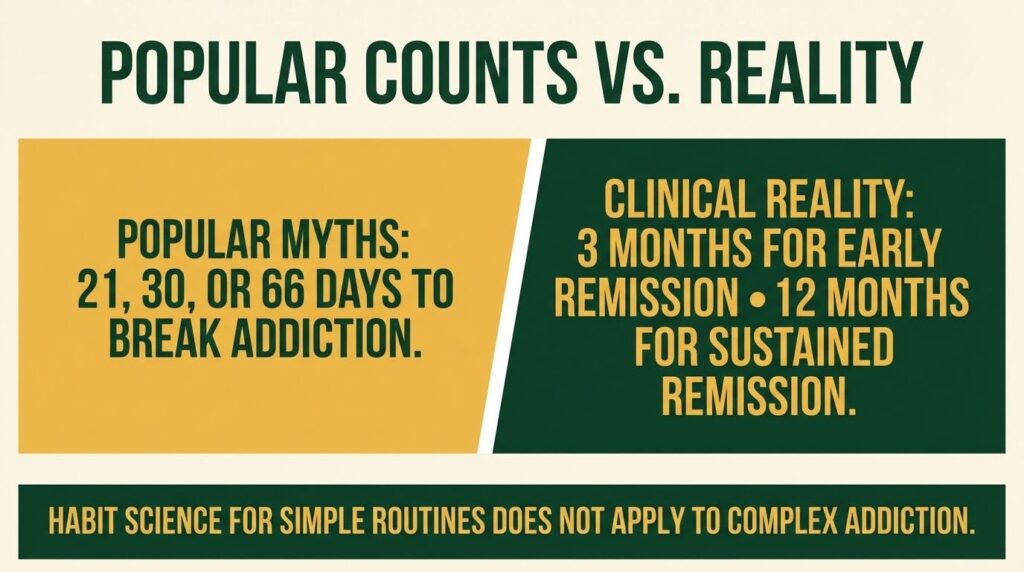
The long-term relapse study found that the mean time in full remission before relapse was about 3.6 years, with a range extending to more than 22 years. Recovery vigilance is not just an early-stage concern.
As life stabilizes, recovery can quietly lose its central place. Meetings become less frequent. Therapy ends. The daily practices that once felt essential start to feel optional. This gradual drift is itself a warning sign.
Healthy coping skills for addiction over the long term include:
- Keeping some level of recovery engagement active, even when things are going well
- Noticing when “I’m fine now” thinking starts to erode boundaries
- Reassessing routines after major life changes such as a new job, a move, or a relationship shift
- Addressing new stressors early rather than absorbing them silently
- Returning to more intensive support quickly after any lapse
Ongoing outpatient therapy or aftercare following initial treatment is recommended in clinical guidance specifically because addiction recovery is a long-term process, not a finite episode.
Continuing care is not a sign of weakness. It is one of the healthiest coping skills for addiction recovery available.
How These Skills Work Together?
No single coping skill is enough on its own. A breathing exercise will not protect someone who is sleep-deprived, isolated, skipping treatment, and returning to high-risk environments.
Conversely, a person with a stable routine, good sleep, regular support contact, and honest self-monitoring is far better protected than someone who knows many techniques but uses none of them consistently.
The strongest evidence across relapse prevention research points to a layered system: structured routine, active social support, consistent self-care, early warning sign recognition, cognitive-behavioral coping, and ongoing recovery engagement.
These work together because they address both the acute moments of crisis and the slower, quieter conditions that make those moments more likely.
Recovery is not about eliminating discomfort. It is about building the capacity to meet discomfort without automatically reaching for a substance. That capacity is built skill by skill, day by day, through practice.
If you are ready to build that foundation with professional support, Mosaic’s addiction recovery services can help you take the next step.