Substance Abuse: Is Addiction Genetic or Environmental?
If you have a family history of substance abuse, you may wonder whether addiction was passed down to you.
Research shows that about half of the risk for substance use disorders comes from genetic factors, while the other half stems from environment, stress, and life experience.
This article breaks down what science actually tells us about genetic predisposition to addiction and how the environment shapes the rest.
Is Addiction Genetic? What the Research Shows
The question “is addiction genetic?” does not have a simple yes or no answer. It is both. Decades of twin and adoption studies consistently place the heritability of substance use disorders at roughly 50%.
A meta-analysis of 18 studies found that alcohol use disorder heritability sits at about 49%, with a tight confidence interval of 0.47 to 0.54. That estimate held steady whether researchers looked at twins raised together or children raised by adoptive families.
Broader reviews across multiple substances tell a similar story. Is drug addiction genetic in the same way? Yes, to a comparable degree.
Is alcohol addiction genetic at a different rate? Not really. Heritability hovers around 50% for most substance use disorders, though nicotine and opioid disorders show slightly more substance-specific genetic influence on top of the shared risk.
But here is the part that matters most: heritability is a population-level statistic. It tells us how much genetic variation explains differences across a group.
It does not tell any single person that they are destined to develop a substance use disorder. The remaining 50% of risk comes from environmental exposures, developmental timing, trauma, peer influence, and access to substances.
The General Addiction Risk Factor
One of the more striking findings in recent years is that there is a shared genetic vulnerability that cuts across substances.
Researchers using a method called Genomic Structural Equation Modeling found a single addiction risk factor that captures genetic liability common to problematic alcohol use, opioid use disorder, cannabis use disorder, and tobacco use disorder.
What makes this finding especially interesting is that the shared genetic factor persists even after researchers remove the genetic influences on normal, non-problematic substance use.
In other words, the genes that raise your risk for developing a disorder are not simply the same genes that make you more likely to try a drink or a cigarette. There is something genetically distinct about the transition from use to disordered use.
Among the substances studied, opioid and cannabis use disorders tend to load most heavily onto this shared factor, while problematic tobacco use loads the lowest.
This pattern suggests that the biology of addiction vulnerability is not identical across every substance, even though a large portion of risk is shared.
How Much of Addiction Is Genetic Versus Environmental?
So how much of addiction is genetic, exactly? The best current answer is about half. But that number deserves context.
Twin-based heritability captures all genetic variation, including rare variants and gene-gene interactions. When scientists look only at common genetic variants measured by modern DNA chips, the numbers drop. For tobacco use disorder, SNP-based heritability falls between roughly 5% and 15%.
This gap does not mean the twin studies were wrong. It means that current technology captures only a slice of the full genetic picture.
The environmental half of the equation is just as real and arguably more actionable. Environmental risk factors include:
- Early life adversity and childhood trauma
- Chronic stress and lack of social support
- Neighborhood substance availability and peer norms
- Policy environments such as prescribing practices and alcohol regulations
- Developmental timing of first exposure
- Co-occurring mental health conditions like ADHD and depression
- Major disruptions such as the COVID-19 pandemic, which increased relapse risk through isolation and service disruption
These factors do not simply add to genetic risk. They interact with it. A person with high genetic liability who grows up in a stable, low-stress environment with limited substance access may never develop a disorder.
A person with moderate genetic risk who faces repeated trauma and easy access to drugs may develop one quickly. The question is not really “is addiction genetic or environmental?” It is how and when these forces combine.
Is There a Genetic Predisposition to Addiction Across Substances?
Yes, and the evidence for a genetic predisposition to addiction that spans multiple substances is now strong.
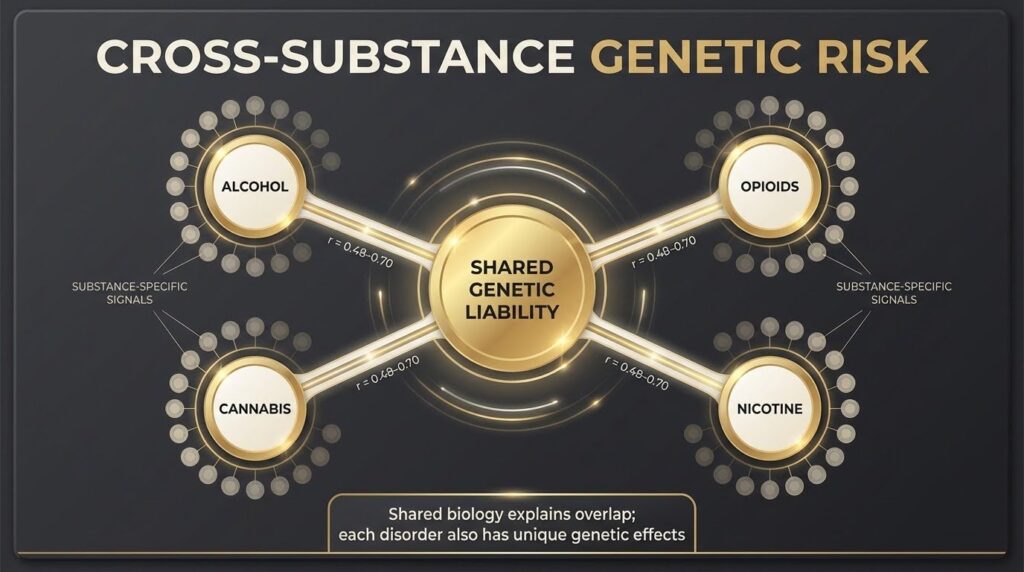
Cross-substance genetic correlations among problematic alcohol use, opioid use disorder, cannabis use disorder, and nicotine use disorder typically range from 0.48 to 0.70 in European-ancestry samples.
That means a large chunk of the genetic risk for one substance use disorder overlaps with the risk for others.
A cross-ancestry study of tobacco use disorder found genetic correlations of 0.74 to 0.84 across different population groups, suggesting that the broad genetic architecture of addiction risk is similar worldwide, even when specific variant frequencies differ.
This shared biology makes sense when you consider what addiction does in the brain. Functional genomic studies show that the genes involved in cross-substance risk are most active in neuronal cells across the amygdala, cortex, hippocampus, hypothalamus, and thalamus.
These are brain regions tied to reward learning, stress response, decision-making, and emotional regulation. The cell-type enrichment data point to a biologically coherent system, not a random scattering of genetic effects.
Substance-Specific Genetic Effects
Beyond the shared factor, each substance also has its own genetic fingerprint. A study of over 2.2 million people found that after accounting for shared externalizing traits like impulsivity and risk-taking, substance-specific genetic signals still predicted individual disorders.
A residual polygenic score for opioid use disorder, for example, best predicted opioid use disorder specifically, not other substance use disorders.
This layered architecture matters for research. It means scientists can build both broad risk scores that capture general addiction vulnerability and narrow scores that capture substance-specific biology. Neither alone tells the full story.
The Externalizing Connection
Addiction does not exist in a genetic vacuum. Much of the shared genetic risk for substance use disorders overlaps with a broader set of traits called the externalizing spectrum.
This includes impulsivity, risk-taking, conduct problems, and ADHD. Twin and family studies show that a generalized genetic liability for externalizing behaviors spans multiple forms of behavioral difficulty, with substance use disorders as one expression.
This developmental co-aggregation appears in both men and women and tracks from adolescence into adulthood. It helps explain why people with ADHD or conduct disorder in childhood face higher substance use disorder risk later.
The genetic overlap is real, and the environmental pathway from early behavioral difficulty to later substance involvement is well documented.
But externalizing is not the whole story. Recent multivariate analyses show that even after removing shared externalizing variance, substance use disorders retain unique genetic associations with internalizing conditions like depression and anxiety. Multiple pathways lead into addiction, and they are not all the same.
Can Genetic Testing Predict Addiction?
Not yet, at least not in a clinically useful way. Current polygenic risk scores for substance use disorders explain only a small fraction of who will develop a problem. A large multi-ancestry study of over one million people explicitly cautioned that their findings “do not apply to prognostication of future disease risk.”
There are several reasons for this gap between discovery and prediction. The genetic architecture of addiction is highly polygenic, meaning thousands of variants each contribute a tiny amount of risk. Current scores capture only common variants and miss rare ones.
And scores trained mostly on European-ancestry populations perform worse in other groups, raising serious equity concerns.
| Challenge | Current Status |
|---|---|
| Variance explained by polygenic scores | Typically 1 to 5% for individual substance use disorders |
| Cross-ancestry performance | Reduced in non-European populations due to training bias |
| Clinical readiness | Not recommended for individual risk prediction |
| Best current proxy for genetic risk | Family history of substance use disorders |
Some promising work is underway. Multi-ancestry training improves score performance in underrepresented groups. Post-hoc ancestry calibration, tested in African American cohorts, reclassified over a third of individuals in the highest risk group and sharpened prediction.
Transdiagnostic scores that capture shared psychiatric liability show better portability across populations than disorder-specific scores.
Still, for now, family history remains the most practical and equitable indicator of genetic vulnerability. It captures both inherited biology and shared family environment, and it costs nothing.
What About Pharmacogenetics and Treatment?
One area where genetics might soon affect treatment is pharmacogenetics, the study of how genetic variants influence medication response. The most studied example in addiction medicine involves the OPRM1 gene and naltrexone, a medication used for alcohol use disorder.
A 2020 meta-analysis of randomized trials found that evidence for the OPRM1 variant rs1799971 predicting naltrexone response remained inconclusive. Study designs varied, outcomes differed, and no clear, reliable signal emerged.
A more recent prospective study of 100 patients receiving extended-release naltrexone found that the OPRM1 variant did seem to matter, but in an unexpected way.
Carriers of one genotype benefited more from the medication, while others appeared to need stronger psychosocial support. The study also found that motivation interacted with genotype, suggesting that the relationship between genes and treatment response is not purely pharmacological.
This is a promising lead, but the study was small and not randomized. Routine genetic testing before prescribing naltrexone is not supported by current evidence.
What clinicians can do right now is prescribe evidence-based medications for alcohol and opioid use disorders based on clinical presentation, and pair them with psychosocial support for everyone.
Why This Matters for You and Your Family?
Understanding that addiction is roughly half genetic and half environmental changes how we should think about risk and responsibility. If substance use disorders run in your family, you are not doomed. You carry higher statistical risk, but that risk plays out through environment, choices, timing, and support systems.
Family history is worth knowing. It is the single best available proxy for genetic vulnerability, and it can guide earlier conversations about risk, smarter prevention strategies, and faster access to help when problems start.
At the same time, environmental factors are the most modifiable part of the equation. Access to treatment, stable housing, trauma-informed care, strong social connections, and sensible substance policies all reduce the chance that genetic vulnerability turns into a clinical disorder.
Genetics is not destiny. It is probability. And probability can be shaped.
If you or someone you love is struggling with substance use, reaching out for professional support is the most important step you can take. Learn more about our available programs through Mosaic Behavioral Health Center’s website and start the conversation today.