

How Does CBT for Substance Abuse Help Prevent Relapse?
Cognitive behavioral therapy for substance abuse is one of the most studied and widely used treatments in addiction care.
Research shows that CBT helps prevent relapse by teaching people to recognize triggers, challenge the thoughts that lead to use, and practice coping skills before high-risk moments escalate.
This article explains exactly how CBT works, which techniques matter most, and why the evidence supports it as a core part of recovery.
How CBT for Substance Abuse Targets the Relapse Process?
Relapse rarely happens without warning. It usually begins long before a person picks up a substance, with a shift in mood, a familiar place, a stressful conversation, or a thought that quietly gives permission to use. Cognitive behavioral therapy for addiction works by making that process visible and interruptible.
The core idea is straightforward. Substance use is partly a learned behavior, maintained by reinforcement, emotional cues, and automatic thinking.
CBT does not treat addiction as a willpower problem. Instead, it treats it as a sequence of observable events that can be identified, slowed down, and changed.
At the center of that sequence is a chain that looks something like this: a trigger appears, an automatic thought follows, an emotional reaction builds, craving rises, and substance use occurs.
CBT targets each link in that chain. It teaches people to notice triggers earlier, interpret cravings more accurately, and respond with practiced alternatives rather than automatic use.
A foundational review of CBT for substance use disorders describes the approach as a family of interventions united by a focus on overcoming the reinforcing effects of psychoactive substances through cognitive, motivational, and skills-building methods.
That description matters because it signals something important: CBT is not one technique. It is a coordinated system of skills, and its relapse-prevention power comes from how those skills work together.
One of CBT’s most clinically significant strengths is durability. Because it is skills-based rather than insight-based alone, the benefits can continue after formal therapy ends.
A person who has learned to recognize their personal triggers, challenge permission-giving thoughts, and use a coping plan does not lose those abilities when sessions stop. That is a structural advantage in a chronic condition like addiction, where relapse risk extends well beyond the treatment period.
The Core CBT Techniques for Addiction
Self-Monitoring: Making Patterns Visible
Self-monitoring is one of the most practical tools in CBT and addiction treatment. Patients use thought records, craving logs, and mood diaries to track what happens before, during, and after a craving or use episode. Over time, patterns emerge that would otherwise stay invisible.
A person might notice that cravings spike on Sunday evenings, after conflict with a family member, or when they are tired and alone.
That pattern is not obvious in the moment. It becomes clear only when tracked consistently. Once it is visible, it becomes preventable.
Self-monitoring also connects directly to newer digital treatment models. Recent trials of digital CBT for alcohol use disorder included app-based diary functions that tracked alcohol consumption, craving, and mood, with clinician dashboards that flagged rising risk.
The classic CBT diary has become the conceptual foundation for modern digital therapeutics and remote relapse monitoring.
Trigger Recognition and Functional Analysis
CBT distinguishes between external triggers, such as people, places, and times associated with past use, and internal triggers, such as anxiety, loneliness, shame, boredom, and anger. Both matter. Both can drive relapse.
Functional analysis goes deeper than labeling triggers. It asks what need the substance was serving. Was it numbing emotional pain? Reducing social anxiety?
Providing energy or sleep? Without understanding that function, relapse prevention stays superficial. With it, the therapist and patient can design targeted alternatives.
A common shortcut in addiction treatment is telling people to simply avoid triggers. That advice is incomplete. Many triggers cannot be avoided.
Stress, painful memories, and social cues are part of ordinary life. Effective CBT combines avoidance where possible with coping where avoidance is not realistic.
Cognitive Restructuring: Changing What Cravings Mean
Relapse is often driven not just by craving but by the thoughts that surround it. CBT for addiction directly targets automatic thoughts and substance-related beliefs that increase relapse risk.
Common examples include:
- “I’ve already messed up today, so I might as well use.”
- “One drink won’t matter.”
- “I can’t handle this craving.”
- “I deserve this after a hard day.”
- “If I say no, people will reject me.”
These thoughts are not trivial. They compress long-term consequences and magnify short-term relief. Cognitive restructuring teaches patients to identify a thought, test it against evidence, and replace it with a more balanced alternative.
For example, “I can’t tolerate this urge” becomes “This urge is uncomfortable, but urges rise and fall. I’ve gotten through them before.”
One of CBT’s most underappreciated functions is what happens after a lapse. A single slip can become a full return to uncontrolled use when it is interpreted as total failure.
CBT weakens that cascade by teaching people that a lapse is a data point, not a verdict. That cognitive shift is often what separates a brief slip from a prolonged relapse.
Coping Skills Training
Knowing a trigger exists is not enough. A person also needs a practiced response ready when that trigger appears. Coping skills training builds exactly that.
Skills vary by patient but commonly include urge surfing, delay strategies, refusal scripts, leaving high-risk situations, calling a support person, grounding techniques, problem solving, and scheduling sober activities.
The goal is not to eliminate craving but to make non-use behaviorally possible by giving people something to do instead.
Research on CBT4CBT, a web-based CBT program with a strong evidence base, highlights an important point: treatment may improve outcomes not just by increasing the number of coping skills a patient knows, but by improving the quality and actual use of those skills under pressure.
Skills need to be practiced until they are usable in a high-risk moment, not just understood in a calm session.
Relapse Prevention Planning
Relapse prevention is not a late-stage add-on in CBT. It is a central organizing feature. Patients work with their therapist to build a structured plan that includes their top triggers, early warning signs, coping strategies, support contacts, and a step-by-step response for if a lapse occurs.
The logic is that high-risk situations are inevitable. Prevention depends on recognizing risk early, slowing the sequence, applying a preplanned response, and returning to recovery behavior quickly after any slip.
CBT converts relapse prevention from a vague aspiration into a set of pre-rehearsed behaviors.
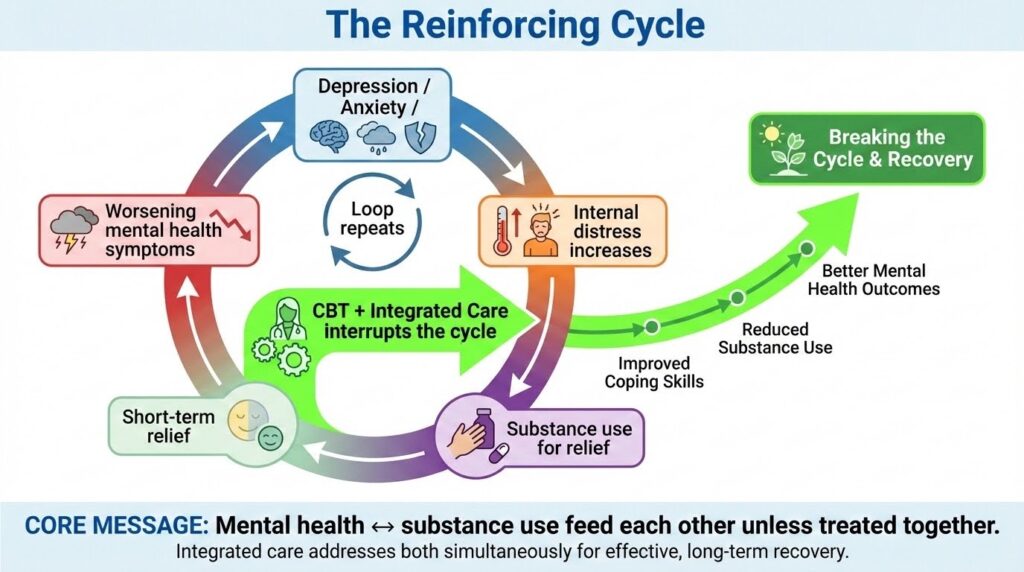
How CBT and Addiction Treatment Work Together With Co-Occurring Conditions?
For many people, relapse is not driven by substance cues alone. It is driven by untreated depression, anxiety, trauma, or other mental health conditions that create internal pressure to use. This is where integrated treatment becomes essential.
A review of integrated treatment for substance use and psychiatric disorders found that treating both conditions simultaneously is consistently superior to treating them separately or in uncoordinated parallel care.
The reasoning is direct: untreated psychiatric symptoms can trigger substance use, and substance use can worsen psychiatric symptoms. Leaving one untreated while addressing the other leaves a major relapse driver in place.
A 2024 umbrella review of psychosocial interventions for adults with substance use disorder and co-occurring mental health conditions confirmed that integrated, coordinated care generally outperforms treating one condition alone. This is one of the most important higher-level findings in the current evidence base.
PTSD and substance use disorder is one of the most clinically difficult combinations. A 2022 systematic review and meta-analysis that included 27 studies and 2,849 participants found that trauma-focused CBT-based approaches improved PTSD symptom severity compared with addiction treatment alone, and some evidence suggested delayed benefits in reduced alcohol use at six to thirteen months.
The review also found that dropout was high, which is a real-world limitation that matters for how treatment is designed and delivered.
The practical implication is clear. If PTSD symptoms improve, the patient has fewer internally driven triggers for substance use. But treating trauma alone is not enough. Direct addiction-focused relapse prevention remains necessary alongside it.
What the Evidence Says About CBT for Addiction?
The evidence base for CBT and addiction is broad and consistent. A review of CBT for substance use disorders describes it as having demonstrated efficacy both as a standalone treatment and in combination with other approaches, with evidence supporting durability of effects over time.
A 2025 systematic review and meta-analysis published in *Psychological Medicine* compared digital and face-to-face CBT for alcohol use disorder across 25 randomized controlled trials with 2,065 participants. For drinking quantity, digital CBT showed a significant effect with a standardized mean change ratio of 1.21.
For drinking frequency, both digital and face-to-face CBT produced significant reductions, with face-to-face showing a stronger effect size.
A separate randomized study of a CBT-based digital therapeutic for alcohol use disorder enrolled 30 outpatients and found that the digital group, who received 84 video-based CBT sessions through a mobile app over 12 weeks, achieved abstinence during weeks nine through twelve at a rate of 73.3 percent, compared with 30.8 percent in the face-to-face control group.
The digital CBT group also showed significantly greater reductions in risky drinking, craving, and anxiety.
These findings matter because they show that CBT’s core mechanisms, self-monitoring, skills rehearsal, and structured feedback, translate effectively into digital formats.
The underlying logic of CBT does not change when delivered through an app. If anything, digital delivery intensifies it by making monitoring and coping support available in real time rather than only during weekly sessions.
SAMHSA’s guidance on substance use treatment reinforces that whole-patient treatment combining medication with counseling and behavioral therapies provides the strongest foundation for recovery.
For opioid use disorder in particular, medication is often indispensable, and CBT works best as a complement to it rather than a substitute.
Why CBT Prevents Relapse: A Summary of the Mechanisms
The table below shows how each CBT mechanism targets a specific point in the relapse process.
| Relapse pathway | CBT target | How it helps |
|---|---|---|
| Unnoticed risk escalation | Self-monitoring | Earlier recognition of warning signs |
| Cue-triggered automatic use | Trigger analysis | Anticipatory planning before exposure |
| Permission-giving thoughts | Cognitive restructuring | Reduces impulsive or rationalized use |
| No alternative to using | Coping skills training | Builds practiced non-use responses |
| Lapse becomes full relapse | Lapse management | Limits escalation after a slip |
| Psychiatric symptoms drive use | Integrated CBT | Fewer internal relapse triggers |
| Risk returns after treatment ends | Skills generalization | Sustained self-management over time |
The deeper point is that CBT does not prevent relapse by eliminating craving. It prevents relapse by making the process that leads to use more visible, more predictable, and more interruptible.
That is a more honest and more useful framing than promising that therapy will remove all risk.
CBT Works Best as Part of a Broader Recovery Plan
The current evidence does not support treating CBT as a complete solution on its own. Substance use disorders are chronic and multifactorial.
The most reliable outcomes come from coordinated care that may include medication, contingency management, peer support, telehealth, and wraparound services alongside CBT.
Contingency management is a good example of a complementary approach. It uses incentives to reinforce abstinence and treatment attendance. CBT builds the internal skills needed to sustain gains after incentives end. Together, they address both capability and motivation.
Telehealth delivery also extends CBT’s reach. A feasibility study of relapse prevention group therapy delivered via videoconferencing found it acceptable and practical for both participants and providers, and telehealth for SUD treatment can reduce barriers related to transportation, geography, and stigma that often lead to treatment dropout and relapse.
The most defensible current position is that CBT is a high-value, evidence-based core treatment whose relapse-prevention power increases when it is coordinated with medication where appropriate, integrated care for co-occurring conditions, and tools that support monitoring and continuity between sessions.
If you are looking for structured, evidence-based support for substance use or co-occurring mental health concerns, speaking with our qualified clinician is a strong first step. Reach out to explore Mosaic’s outpatient treatment options and find the right level of care for where you are right now.