

How Long Does It Take to Break an Addiction? Timeline & Recovery
Breaking an addiction is one of the hardest things a person can do, and the timeline is rarely what popular culture suggests.
Research shows there is no single day count that “breaks” addiction: recovery unfolds across phases spanning days, months, and often more than a year.
This article walks you through what the science actually says about each stage, so you can set realistic expectations and build a plan that works.
How Long Does It Take to Break an Addiction?
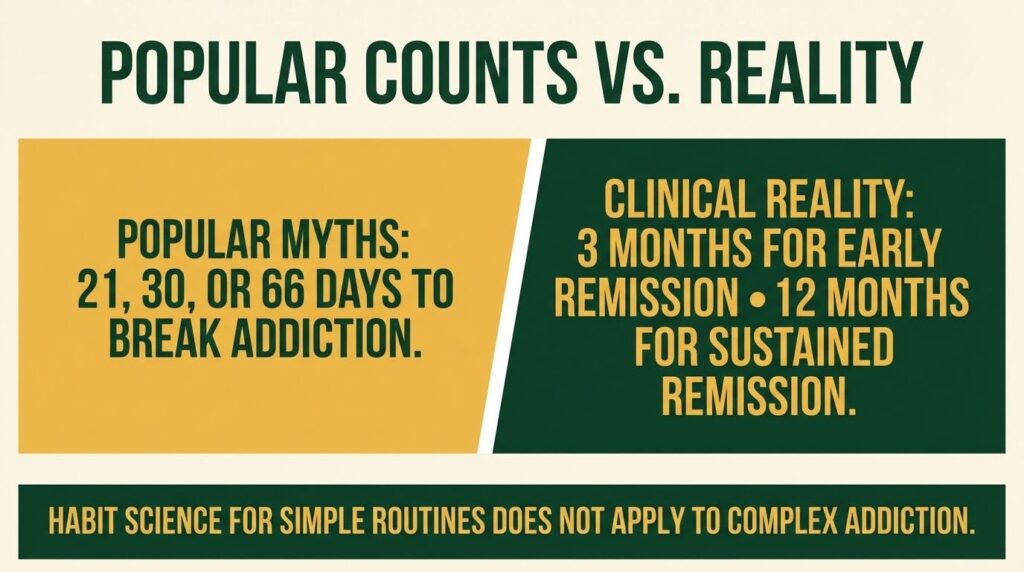
There is no universal number of days that ends an addiction. DSM-5 criteria define early remission as at least three months without meeting substance use disorder criteria (except craving), and sustained remission requires at least twelve months.
The popular claims of 21, 30, 66, or 90 days each come from different sources and track different things, none of which map cleanly onto addiction recovery.
Understanding why those numbers fall short, and what the evidence actually shows, is the first step toward building a realistic recovery plan.
The Addiction Timeline: What Each Phase Looks Like?
Recovery does not happen in a straight line. It moves through overlapping phases, each with its own risks and goals.
Days 1 to 14: Acute Withdrawal
The first phase is medical stabilization. Acute withdrawal begins almost immediately after stopping or sharply reducing use. Symptoms vary by substance but can include tremor, sweating, nausea, pain, and insomnia. For alcohol, severe cases carry the risk of seizures or delirium tremens.
This phase typically resolves within days to a few weeks, but clearing acute withdrawal is not the same as recovering from addiction.
The U.S. Surgeon General’s Report on alcohol, drugs, and health is explicit on this point: withdrawal management is a bridge into treatment, not a standalone endpoint. Treating detox as the finish line is associated with rapid relapse.
Standard care pathways during this phase include medically supervised withdrawal lasting three to seven days, sometimes longer when medical or psychiatric complications exist.
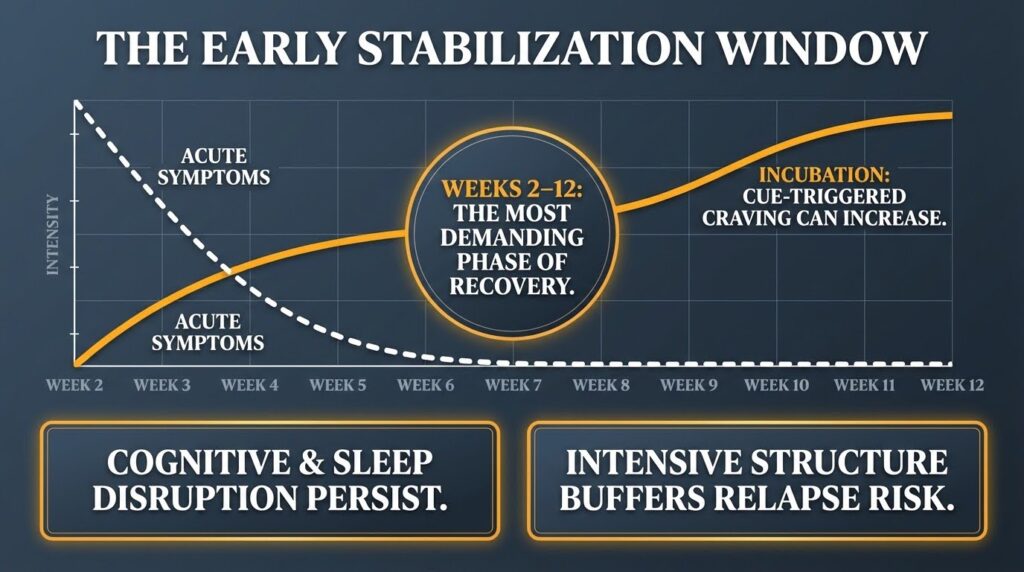
Weeks 2 to 12: Early Stabilization
This is one of the most demanding stretches of the addiction timeline. Cognitive function, sleep, and mood can all remain disrupted well after acute symptoms fade.
Craving does not simply decline with time. Research shows it can actually increase during early abstinence, a process called incubation, where cue-triggered urges grow stronger rather than weaker as days pass.
The DSM-5 work group retained craving as a criterion that can persist even during remission, precisely because it does not resolve on a fixed schedule. Three months marks the threshold for early remission, but that milestone excludes craving by design.
Intensive structure during this phase, whether residential care, intensive outpatient programs running nine or more hours per week, or daily mutual-help attendance, helps buffer the high relapse risk. The “90 meetings in 90 days” practice used in 12-step communities is a good example of this kind of scaffolding.
Recovery providers describe it as a way to build daily accountability and connection during a period of intense emotional turbulence. It is a support structure, not a cure, and research on this practice frames it explicitly as a foundation for the early window, not an endpoint.
Months 4 to 6: Protracted Withdrawal Risk
Many people are surprised to find that months four through six can feel harder than the first few weeks.
This is the window most associated with post-acute withdrawal syndrome (PAWS), a cluster of symptoms including negative mood, sleep disturbance, anhedonia, irritability, cognitive difficulties, and craving.
A systematic review of PAWS in alcohol use disorder found that these symptom clusters can persist four to six months or longer and are linked to neurobiological changes in reward circuits and stress systems. The brain is still recalibrating.
Sleep problems and low mood during this period are not signs of failure; they are signs that the nervous system is still healing, and they need active management.
Pharmacotherapy where indicated, cognitive-behavioral relapse prevention, sleep-focused interventions, and continued environmental restructuring are all critical during this phase.
Months 6 to 12: Consolidation
Relapse risk may begin to decline during this stretch for people who maintain consistent support. Simple protective routines, such as taking a daily medication at the same time each morning or checking in with a sponsor after a set trigger, can start to feel more automatic.
This is where the “66 days” figure from habit science becomes useful in a limited way. A systematic review of health-behavior habit formation found a median of about 59 to 66 days for simple, cue-anchored behaviors to reach subjective automaticity, with a range of 4 to 335 days.
Only a minority of participants in some studies reached preset automaticity thresholds at all. These findings apply to building simple routines like drinking water after breakfast, not to ceasing a complex, neurologically embedded addictive behavior.
The 66-day figure is a useful planning horizon for installing small protective habits, not a clock for extinguishing addiction.
Cue reactivity in brain circuits including the ventral striatum, amygdala, and prefrontal cortex remains a real risk factor throughout this phase. Neuroimaging research consistently shows that drug-related cues activate these circuits and that the strength of that response predicts relapse risk across substances.
12 Months and Beyond: Sustained Remission
Reaching twelve months without meeting substance use disorder criteria (other than craving) marks what the DSM-5 calls sustained remission.
This is a meaningful milestone. Relapse hazard is lower, and recovery capital, meaning stable housing, employment, and relationships, becomes the dominant protective factor.
But sustained remission is not immunity. Cue-triggered vulnerability can persist. Long-term maintenance of medication where indicated, continued engagement with support networks, and a clear plan for high-risk situations all remain important.
Where the Popular Day Counts Actually Come From?
It helps to understand why these numbers circulate so widely, and what they actually measure.
- 21 days traces back to plastic surgeon Maxwell Maltz’s 1960s observations about how long patients took to adjust psychologically to changes in their appearance. It was never a measure of addiction remission, habit automaticity, or cue-reactivity decline. Contemporary behavioral scientists are clear that habit formation has no universal deadline.
- 30 days reflects the length of a residential program cycle or insurance coverage period, not a neurobiological transition point. Many people are still in early stabilization or entering the protracted withdrawal window at day 30.
- 66 days comes from health-behavior research on simple routines. It is a median, not a finish line, and it does not apply to addiction cessation.
- 90 days is a pragmatic support scaffold from mutual-help communities. It overlaps usefully with the DSM early-remission threshold and the high-risk early window, but recovery providers are consistent that it should be framed as a beginning, not an endpoint.
What Happens in the Brain During Recovery?
The neurobiology of addiction explains why short timelines are not enough.
Drug-related cues activate mesolimbic and prefrontal circuits long after the last use. A 2025 randomized controlled trial found that a short-term N-acetylcysteine challenge reduced prefrontal reactivity to cocaine cues in people with cocaine use disorder, showing that these neural responses can be modulated. But longer trials are still needed to connect those biomarker changes to durable clinical outcomes.
Animal research using voluntary-abstinence models, where the drug is available but the animal chooses an alternative reward, found that relapse after voluntary abstinence increased activity in the orbitofrontal cortex and piriform cortex. Inactivating the orbitofrontal cortex reduced relapse behavior, pointing to these circuits as meaningful targets for relapse prevention strategies.
The practical takeaway is that the brain does not simply reset after a fixed number of days. Neuroadaptations that drive craving and impaired control can outlast acute withdrawal by months.
A Realistic Recovery Timeline at a Glance
| Phase | Timeframe | Key risks | What helps |
|---|---|---|---|
| Acute withdrawal | Days 1 to 14 | Medical complications | Supervised detox; medication initiation |
| Early stabilization | Weeks 2 to 12 | High craving; cue reactivity | Intensive structure; daily support; medication |
| Protracted withdrawal | Months 4 to 6 | Mood, sleep, anhedonia | Pharmacotherapy; CBT; sleep intervention |
| Consolidation | Months 6 to 12 | Cue-triggered relapse | Habit-building; continued medication; step-down care |
| Sustained remission | 12 months and beyond | Episodic setbacks | Recovery capital; ongoing support as needed |
Why the Timeline Matters for Real Outcomes?
Getting the timeline wrong has real consequences. Someone who believes addiction is “broken” after 30 days may stop treatment just as protracted withdrawal symptoms are peaking. Someone who hears that 66 days makes sobriety automatic may feel like a failure when cravings return at month three.
Calibrating expectations to a yearlong horizon, with specific phase goals and supports, gives people a much better chance of staying in care through the periods of highest risk.
The SAMHSA treatment guidelines describe a continuum of care that moves from medically managed withdrawal through residential or intensive outpatient programs and into step-down outpatient services, with intensity titrated to risk and progress rather than fixed to a day count.
Recovery is not a sprint to an arbitrary finish line. It is a phased process with a realistic planning horizon of at least twelve months, and often longer, depending on the substance, the person, and the supports in place.
If you or someone you care about is navigating this process, speaking with a specialist can help you match the right level of care to the right phase of recovery. Reach out to our team to explore treatment options and get support that fits where you are right now.