

Insomnia After Quitting Alcohol: Causes, Duration & Sleep Tips
Insomnia after quitting alcohol is one of the most common and frustrating parts of early recovery.
For many people, the most severe sleep problems peak in the first week and begin to ease within two to four weeks, though a meaningful number of people struggle for months or longer.
This article walks through why sleep suffers after you stop drinking, how long insomnia typically lasts, and what the evidence says actually helps.
Insomnia After Quitting Alcohol: What is Happening and Why?
When you drink heavily over time, your brain adapts. It dials down the calming signals and dials up the excitatory ones to stay balanced.
The moment you stop, those excitatory systems run unchecked. The result is hyperarousal: a wired, restless state that makes falling asleep and staying asleep genuinely hard.
Alcohol also reshapes your sleep architecture over time. Research on alcohol and sleep shows that chronic heavy drinking reduces slow-wave sleep, the deep restorative stage, while increasing REM sleep pressure.
REM pressure means your brain pushes harder and earlier into the rapid eye movement stage, producing fragmented, unrefreshing sleep. When you quit, both of these disruptions do not vanish overnight. They linger, sometimes for months.
There is also a circadian component. Heavy drinking destabilizes your internal body clock, making it harder to fall asleep at a consistent time and easier to wake in the early hours.
The Neurochemistry Behind the Sleeplessness
Alcohol works partly by boosting GABA, the brain’s main calming neurotransmitter, and suppressing glutamate, the main excitatory one. With prolonged use, the brain compensates by reducing GABA sensitivity and increasing glutamate activity.
Stopping alcohol suddenly leaves glutamate dominant, which is why withdrawal feels so activating and why sleep feels impossible in those first days.
This imbalance also affects the stress hormone system. The HPA axis, which governs your cortisol response, stays dysregulated for weeks after cessation, keeping arousal levels high at night when they should be falling.
How Long Does Insomnia Last After Quitting Alcohol?
This is the question most people want answered, and the honest answer is: it depends on the phase of recovery.
A comprehensive review of sleep in alcohol use disorder found that 67 percent of detoxified men reported insomnia, with 25 percent experiencing it within the first 48 hours and about 58 percent having at least one night of insomnia within the first six days. That is the acute peak.
Here is a rough timeline based on the research:
- Days 1 to 7: Insomnia is at its worst. Sleep latency is long, total sleep time is short, and awakenings are frequent. REM rebound, where the brain floods into REM sleep it was suppressed from during drinking, adds to fragmentation.
- Weeks 1 to 4: Gradual improvement begins for many people, but sleep remains substantially impaired. A meta-analysis of polysomnographic studies confirmed that total sleep time, sleep efficiency, and slow-wave sleep all remain below normal averages during this window.
- Months 1 to 3: Sleep continuity, meaning how well you stay asleep, often approaches near-normal levels for many people. Subjective complaints, however, frequently persist even when objective measures improve.
- Months 6 to 12 and beyond: Most people achieve functionally acceptable sleep, but a meaningful subset does not. Research tracking abstinent individuals has documented abnormal sleep architecture, including reduced deep sleep and elevated REM percentage, lasting up to 27 months in some cases.
The short answer: for many people, the worst insomnia eases within two to four weeks. Substantial improvement in sleep continuity often comes by one to three months.
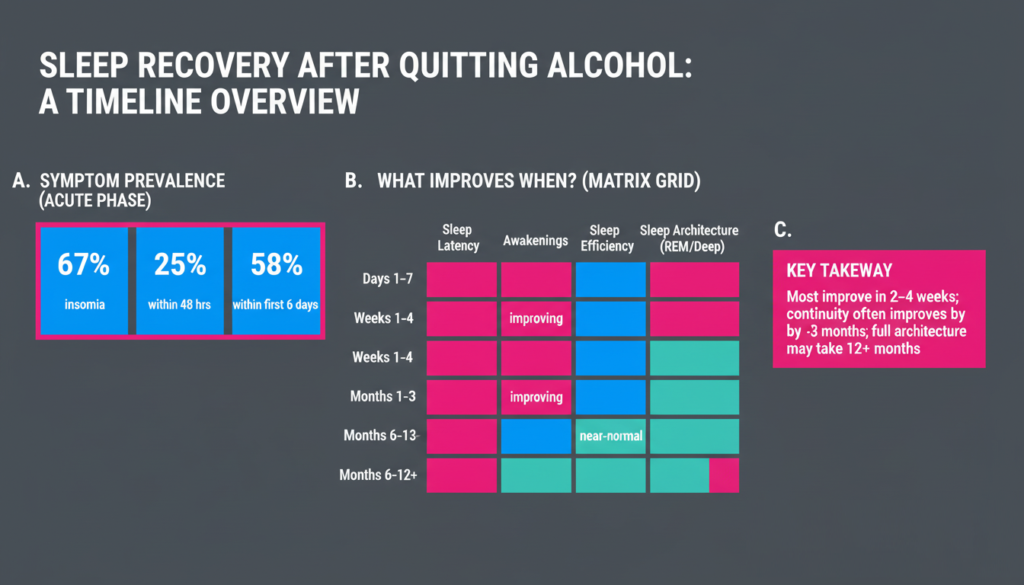
Full normalization of sleep architecture, the deeper structural patterns, can take a year or more and may never fully return for some.
Why Some People Take Longer?
Several factors slow recovery. Comorbid anxiety or depression is a major one, as mood disorders independently disrupt sleep and can amplify insomnia long after alcohol is gone.
Irregular sleep schedules, nicotine use, and untreated sleep disorders like obstructive sleep apnea also extend the timeline. Age matters too: older adults tend to lose deep sleep faster and recover it more slowly.
How Sleep Problems Connect to Relapse Risk?
This is not just about comfort. Poor sleep after quitting alcohol is a genuine relapse risk factor.
Studies show that people who relapse tend to have longer sleep latencies, shorter REM latency, and less deep sleep before they drink again.
A study tracking sleep regularity after inpatient discharge found that a lower Sleep Regularity Index, a measure of how consistent your sleep timing is day to day, predicted relapse within the first 28 days after leaving treatment.
People who relapsed also reported worse subjective sleep quality and longer daytime naps, suggesting a dysregulated circadian pattern.
The mechanism makes sense. Poor sleep increases negative affect, impairs prefrontal regulation, and raises craving. Alcohol then becomes a tempting shortcut to sedation. Treating insomnia is therefore not separate from relapse prevention. It is part of it.
A randomized trial in veterans during early recovery found that participants who achieved insomnia remission, regardless of which treatment they received, had substantially lower alcohol craving for up to six months compared to those who did not. Craving scores were roughly 2.8 versus 9.5 in those groups. That gap matters.
How to Stop Alcohol Insomnia: What the Evidence Supports?
Cognitive Behavioral Therapy for Insomnia
CBT-I is the most evidence-backed treatment for insomnia after quitting alcohol. It targets the behaviors and thought patterns that keep insomnia going: irregular schedules, spending too long in bed awake, and anxious beliefs about sleep.
It works regardless of what originally caused the insomnia, which makes it well suited to the complex picture of alcohol recovery.
A 2025 meta-analysis across the spectrum of alcohol use disorder found that CBT-I reduced insomnia severity significantly compared to control conditions at the end of treatment, with benefits maintained at one to three months and six months. The mean difference in insomnia severity scores was about 5.5 points at post-treatment, which is clinically meaningful.
Digital CBT-I programs have shown particular promise because they remove access barriers. A randomized pilot study of the SHUTi digital program in heavy drinkers with insomnia found that participants using the program had greater reductions in insomnia and also drank less than those in an education control group, with benefits sustained to six months and no adverse events.
The entire trial ran remotely, showing that effective care does not require an in-person clinic.
Practical Sleep Tips for Early Recovery
The following strategies are grounded in the behavioral principles of CBT-I and are appropriate to start in the first weeks after quitting:
- Keep a fixed wake time every day, even after a bad night. This anchors your circadian rhythm.
- Get morning light exposure within an hour of waking. Natural light is one of the strongest signals to your body clock.
- Get out of bed if you have been awake for more than 15 to 20 minutes. Lying awake in bed trains your brain to associate the bed with wakefulness.
- Avoid caffeine after midday and cut out nicotine where possible, as both fragment sleep.
- Keep daytime naps short and early, or skip them entirely. Long naps reduce sleep pressure at night.
- Avoid screens and bright light in the hour before bed to support melatonin release.
- Track your sleep with a simple diary. Noting your bedtime, wake time, and how you felt helps you spot patterns and gives a clinician useful information.
What About Medication?
Medications for insomnia in alcohol recovery require caution. Benzodiazepines are appropriate during acute withdrawal under medical supervision to prevent seizures, but they are not a solution for ongoing insomnia in recovery because of dependence risk.
Trazodone is commonly prescribed, but a narrative review of insomnia treatment in alcohol recovery raised concerns: sleep benefits did not persist at three to six months, and there were signals of increased drinking after stopping the medication. The review recommends against using trazodone routinely in early recovery.
A systematic review of pharmacologic options found mixed and limited evidence for most agents, reinforcing that behavioral therapy should be the backbone of insomnia care in this population.
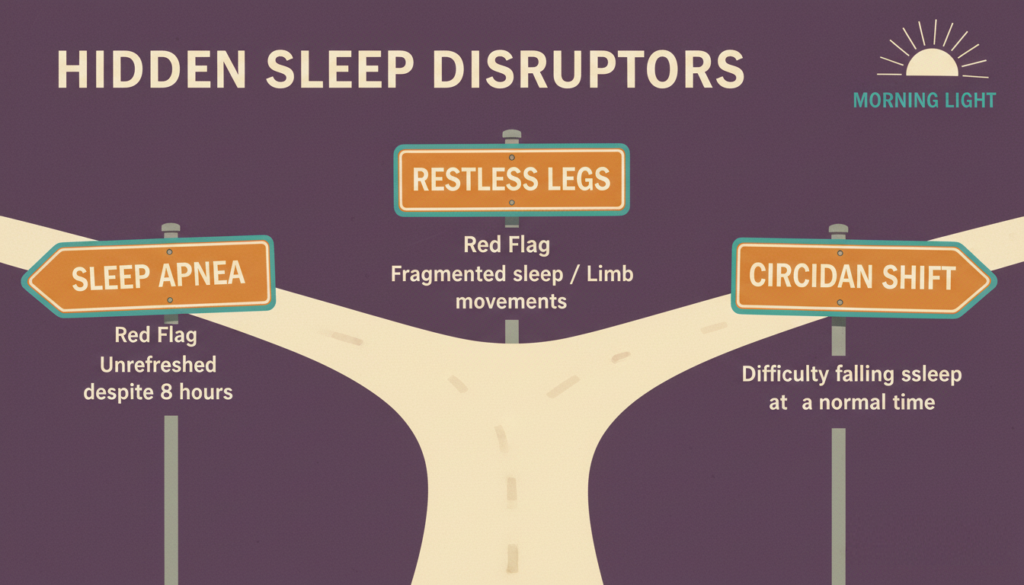
Screening for Other Sleep Disorders
Insomnia after quitting alcohol is sometimes made worse by an underlying sleep disorder that alcohol was masking or worsening.
Obstructive sleep apnea is common in people with alcohol use disorder. Alcohol relaxes the muscles of the throat, worsening breathing during sleep. If you snore loudly, wake gasping, or feel unrefreshed despite adequate time in bed, it is worth asking a doctor about a sleep study.
Restless legs syndrome and periodic limb movements in sleep can also fragment sleep and are more common during early abstinence. Iron deficiency is a treatable contributor, so checking ferritin levels is a reasonable first step.
Circadian rhythm disruption, where your internal clock is shifted or irregular, can cause persistent difficulty falling asleep at a normal time. Morning light therapy and consistent scheduling are the main tools here, and they complement CBT-I well.
What to Expect Over Time?
A staged model fits the evidence best. Think of recovery in three broad phases:
The first phase, roughly the first month, is about stabilizing. Sleep will likely be poor, especially in the first week. The goal is safety, consistency, and starting behavioral strategies early rather than waiting for sleep to fix itself.
The second phase, months one to three, is where many people see real gains in how well they sleep through the night. Subjective complaints may lag behind objective improvement, meaning you might still feel like a poor sleeper even as your sleep data looks better. That gap is normal and tends to close with time.
The third phase, beyond three months, is about consolidating gains and managing residuals. Some people will have fully recovered sleep by six months.
Others, particularly those with mood disorders or irregular schedules, may still notice problems. Booster sessions of CBT-I, continued attention to sleep hygiene, and treatment of any underlying conditions all help during this phase.
The research on sleep architecture recovery shows partial normalization of brain-level sleep markers over 12 months of abstinence, which is encouraging. But it also confirms that complete normalization is not guaranteed within the first year, so patience and ongoing care matter.
Why Treating Sleep Early Makes a Difference?
Waiting for sleep to fix itself is not a good strategy. The evidence is clear that insomnia in early recovery predicts relapse, and that treating insomnia reduces craving and alcohol-related harm even when it does not always change abstinence rates directly.
Starting CBT-I, whether in person or through a digital program, within the first two to four weeks of quitting gives you the best chance of breaking the cycle. Stabilizing your sleep schedule, getting morning light, and keeping the bed for sleep only are low-cost steps you can take today.
If sleep problems persist beyond four to six weeks despite consistent effort, talking to a clinician about a formal CBT-I program or a sleep study is a reasonable next step.
Recovery from alcohol use disorder is hard enough without running on empty. Treating your sleep is not a side project. It is central to getting well.
If you are struggling with sleep, alcohol use, or both, speaking with a specialist can make a real difference. Reach out to Mosaic Behavioral Health to learn about outpatient treatment options that address both mental health and substance use in an integrated, evidence-based way.