

Insomnia After Quitting Marijuana: Causes & Sleep Solutions
Quitting marijuana often triggers severe insomnia that can last for weeks, leaving many people wondering if they’ll ever sleep normally again.
Within 24 to 48 hours of stopping, sleep architecture begins to deteriorate, with total sleep time dropping, awakenings increasing, and vivid dreams disrupting rest, changes that peak around days 2 to 6 and drive many back to using.
This article explains why cannabis withdrawal causes insomnia, what happens to your brain and sleep cycles during recovery, and the evidence-based strategies that actually work to restore sleep without relying on weed.
Why Quitting Weed Causes Insomnia?
Cannabis withdrawal insomnia stems from neurobiological changes in your brain’s sleep regulation systems. When you use marijuana regularly, THC acts on CB1 receptors throughout your brain, initially promoting sedation and altering sleep stages.
Over time, chronic exposure leads to tolerance, meaning the sleep-promoting effects fade while your brain adapts to constant THC stimulation.
When you stop using, your endocannabinoid system suddenly shifts from chronic external stimulation to relatively low internal signaling.
This abrupt change disrupts the neural circuits that control arousal, REM sleep, and deep slow-wave sleep. Polysomnography studies show that heavy users experience reduced total sleep time, lower sleep efficiency, increased wake time after sleep onset, and a characteristic REM rebound, shortened REM latency and increased REM percentage, within the first nights of abstinence.
The severity correlates directly with prior use patterns. Heavier users who consumed marijuana five or more times per week show more pronounced sleep disturbances, including increased periodic limb movements that correlate with the quantity and duration of prior use.
These objective changes align with subjective complaints of insomnia and strange dreams, which occur in 32 to 76 percent of people during withdrawal.
How Cannabis Withdrawal Disrupts Sleep Architecture?
Understanding what happens to your sleep stages during withdrawal clarifies why insomnia feels so severe and why certain interventions work better than others.
Acute Effects Versus Chronic Tolerance
In occasional users, acute THC can shorten the time to fall asleep and may increase slow-wave sleep, the deepest and most restorative stage. However, systematic reviews reveal that these effects are inconsistent across studies and depend heavily on dose, cannabinoid composition, and individual factors.
More importantly, chronic daily use leads to tolerance, the sleep-inducing benefits diminish over time, and sleep efficiency often worsens despite continued use.
Interestingly, tolerance to THC’s REM-suppressing effects develops more slowly than tolerance to its sedative effects. This asymmetry becomes critical during withdrawal: when you stop, the muted REM suppression unmasks a strong REM rebound, while the tolerance to slow-wave enhancement leaves deep sleep depleted.
The result is a mixed picture of longer sleep onset, more awakenings, less total sleep, reduced slow-wave sleep, and early-phase REM instability.
The Withdrawal Timeline
Cannabis withdrawal symptoms typically begin 24 to 48 hours after cessation, peak between days 2 and 6, and can persist for two to three weeks or longer in heavy users. Sleep disturbances follow a dynamic pattern:
- Days 1 to 7: Sleep onset latency increases, wake after sleep onset rises, total sleep time and efficiency drop, and REM rebound appears with shortened REM latency and increased REM percentage.
- Weeks 2 to 4: REM changes tend to decline with continued abstinence, but wake time and reduced slow-wave sleep may persist, causing ongoing nonrestorative sleep and fatigue.
- Beyond 45 days: A subset of individuals continues to experience sleep problems, often reflecting unmasked underlying sleep disorders, behavioral conditioning, or comorbidities rather than lingering receptor changes.
An inpatient polysomnography series tracking 18 heavy users across two weeks of abstinence documented declining total sleep time and sleep efficiency, increasing wake time, declining REM amount over time, and increasing periodic limb movements, all objective markers of the hyperarousal state that characterizes early withdrawal.
The Brain Science Behind Insomnia From Quitting Weed
CB1 Receptor Downregulation and Recovery
Chronic THC exposure downregulates CB1 receptor availability in the brain by approximately 15 to 20 percent compared to non-users.
These receptors are central to regulating arousal, REM-NREM cycling, and homeostatic sleep drive. When you quit, the sudden removal of exogenous THC leaves your endocannabinoid system operating with relatively low signaling capacity, contributing to hyperarousal and sleep fragmentation.
Importantly, PET imaging studies in cannabis-dependent individuals show that CB1 receptor availability begins to normalize rapidly, group differences between users and controls disappear after just two days of abstinence and remain absent at 28 days.
However, lower receptor availability at day two correlates inversely with withdrawal severity, linking the endocannabinoid system directly to symptom burden during the acute phase.
This rapid receptor normalization suggests that prolonged insomnia beyond four to six weeks is less likely driven by lingering CB1 downregulation and more by behavioral conditioning, pre-existing sleep vulnerabilities, and comorbidities.
Orexin and Arousal Systems
The orexin (hypocretin) system stabilizes wakefulness and coordinates arousal with reward and motivation pathways. Orexin signaling has been implicated in sleep disruption and craving across substance use disorders.
While not yet tested specifically in cannabis withdrawal, blocking orexin receptors improves sleep in chronic insomnia and may attenuate withdrawal and craving in other substance use populations, supporting a bidirectional sleep-addiction framework.
Conditioned Arousal and Coping-Oriented Use
Many people with baseline sleep difficulties initiate and maintain cannabis use as a sleep aid, forming strong conditioned associations between using and falling asleep.
Upon cessation, going to bed without cannabis becomes a cue for “not sleeping,” amplifying withdrawal insomnia and prolonging sleep problems beyond the period explained by receptor normalization alone. This conditioning persists and is a plausible driver of longer-lasting insomnia after quitting.
Evidence-Based Strategies to Sleep Without Weed
The most effective approach to sleeping after quitting weed combines behavioral sleep medicine with circadian interventions, reserving short-term pharmacologic support for acute withdrawal when relapse risk is highest.
Cognitive Behavioral Therapy for Insomnia (CBT-I)
CBT-I is the first-line treatment for chronic insomnia, strongly recommended by the American Academy of Sleep Medicine. It reliably improves sleep initiation, maintenance, and quality, with benefits persisting beyond the treatment period. CBT-I addresses the perpetuating factors of insomnia that outlast the withdrawal window, reducing relapse risk linked to chronic poor sleep.
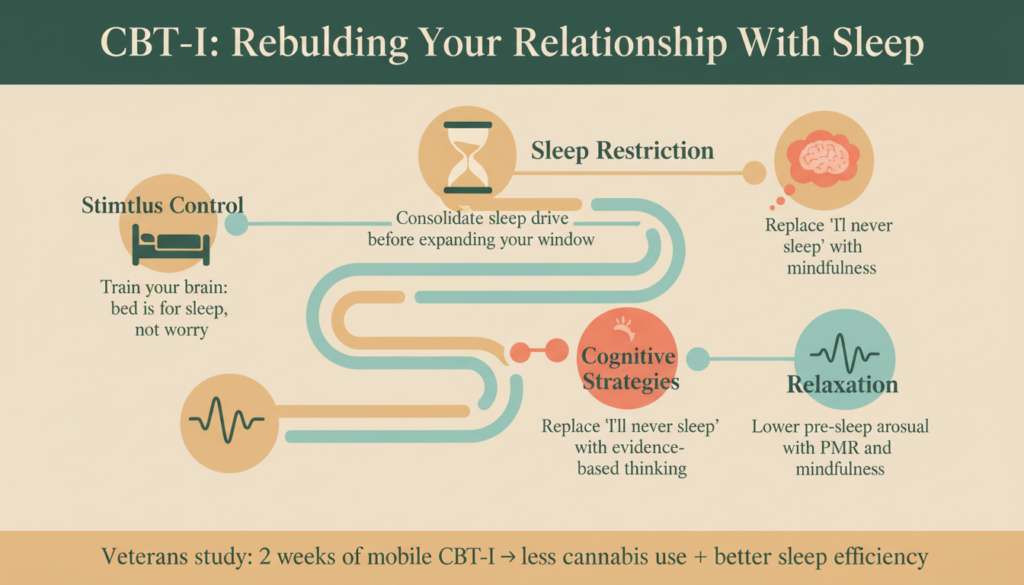
Key components include:
- Stimulus control: Retraining the bed-sleep association by going to bed only when sleepy, leaving bed if awake more than 15 to 20 minutes, and using the bed only for sleep.
- Sleep restriction: Consolidating sleep by limiting time in bed to match actual sleep time, then gradually expanding the window as sleep efficiency improves.
- Cognitive strategies: Reducing catastrophizing and worry about sleep through structured thought challenges.
- Relaxation techniques: Progressive muscle relaxation, breathing exercises, and mindfulness to reduce pre-sleep arousal.
Typically delivered over four to eight sessions in person or via telehealth, CBT-I is the standard against which other treatments should be compared.
A small pilot study in veterans with cannabis use disorder found that two weeks of a mobile CBT-I app was feasible and associated with decreased cannabis use and improved sleep efficiency, supporting the usability of CBT-I content in this population.
Bright Light Therapy and Circadian Entrainment
Bright light therapy is an established treatment for circadian rhythm sleep-wake disorders and a powerful tool during cannabis withdrawal, when irregular schedules and circadian drift are common. Timing is critical:
- To shift sleep earlier (phase advance): Deliver bright light soon after waking in the morning.
- To shift sleep later (phase delay): Deliver bright light in the early evening.
Devices typically provide approximately 10,000 lux for 30 to 60 minutes. Morning bright light within one hour of waking is a pragmatic, low-risk anchor during the withdrawal window, helping to stabilize circadian phase and consolidate sleep drive.
A practical circadian plan includes:
- Obtaining 10,000-lux equivalent bright light for 30 minutes within 60 minutes of waking, either via a light box or 30 to 60 minutes of outdoor sunlight.
- Strictly minimizing evening bright light, especially blue-enriched light, in the last two to three hours before bed.
- Keeping caffeine consumption before early afternoon and avoiding alcohol as a sedative.
- Maintaining a consistent rise time within 30 minutes, even after poor nights, to stabilize anchor times.
Sleep Restriction Protocol
Sleep restriction is a core CBT-I technique that consolidates sleep by matching time in bed to actual sleep time, then gradually expanding the window as efficiency improves.
During withdrawal, this approach counteracts the hyperarousal and fragmentation that characterize early abstinence.
Implementation steps:
1. Calculate average total sleep time from a baseline sleep diary (for example, 5.5 hours).
2. Set time in bed equal to total sleep time plus 30 to 45 minutes (for example, 6 to 6.25 hours), with a fixed rise time.
3. Adjust weekly based on sleep efficiency (total sleep time divided by time in bed):
- If efficiency exceeds 85 percent, increase time in bed by 15 to 30 minutes.
- If efficiency is 80 to 85 percent, hold steady.
- If efficiency is below 80 percent, reduce time in bed by 15 minutes, never below 5 hours.
This consolidates sleep drive during withdrawal hyperarousal and prevents the common mistake of spending excessive time in bed trying to “catch up,” which worsens insomnia.
Pharmacologic Options for Acute Withdrawal Insomnia
Pharmacotherapy should be short-term, symptom-targeted, and adjunctive to behavioral and circadian care. The goal is to bridge the acute withdrawal peak (days 2 to 10) and reduce relapse risk without creating new dependencies.
Gabapentin
A 12-week randomized controlled trial in cannabis-dependent adults found that gabapentin 1,200 mg per day significantly reduced cannabis use, decreased overall withdrawal severity, and significantly improved sleep by Pittsburgh Sleep Quality Index total and components, including sleep efficiency and duration. Executive function and marijuana-related problem scores also improved versus placebo.
Gabapentin can be a reasonable short-term adjunct to CBT-I for patients at low risk of misuse, with the dual potential to improve sleep and reduce cannabis use and withdrawal severity.
However, systematic reviews report gabapentin misuse prevalence around 40 to 65 percent among individuals with prescriptions and 15 to 22 percent in people who misuse opioids. Clinicians should screen for misuse risk, use prescription monitoring, and avoid co-administration with other CNS depressants.
Short-Term Hypnotics
Clinical management guidance recommends supportive care, CBT-I, and optional short-term hypnotics in some settings for withdrawal insomnia:
- Zolpidem: A GABA-A positive allosteric modulator that can target withdrawal-related sleep difficulty. Prior laboratory work noted benefits for sleep during abstinence. Risks include dependence and parasomnias; use for a few nights only.
- Diazepam: May be considered short-term in supervised settings. Risks include sedation, respiratory depression (especially with other depressants), and dependence.
These are not first-line for chronic insomnia but may bridge acute withdrawal to reduce relapse risk when behavioral measures alone are insufficient.
Dual Orexin Receptor Antagonists (DORAs)
For persistent insomnia beyond the acute withdrawal window, dual orexin receptor antagonists such as lemborexant, suvorexant, and daridorexant have the strongest general efficacy and safety profile.
A network meta-analysis of 45 randomized controlled trials found that lemborexant ranked best on three of four polysomnography-measured outcomes at four weeks, with a safety profile broadly similar to other treatments.
Orexin signaling links arousal and reward; suvorexant improved sleep, withdrawal, and craving during buprenorphine taper without a clear misuse signal.
While no cannabis-specific DORA trials exist, these data support consideration of DORAs in recovery-related insomnia when CBT-I and circadian strategies are insufficient, with careful monitoring.
What Not to Use?
Avoid THC-containing products and CBN: Using THC or THC-dominant products to self-manage withdrawal insomnia sustains dependence neuroadaptations and increases relapse risk.
No clinical studies have tested isolated CBN on objectively measured human sleep; human evidence to date mixes CBN with THC, precluding attribution.
An ongoing randomized controlled trial will test isolated CBN 30 mg and 300 mg using polysomnography, but until those results are available, recommending CBN for sleep is premature.
A Phase-Informed Protocol for Sleeping After Quitting Weed
Phase 1: Days 0 to 6 (Acute Withdrawal)
Goals: Contain hyperarousal, protect sleep opportunity, reduce relapse risk.
- Education: Normalize the timeline, symptoms start 24 to 48 hours, peak days 2 to 6, may last two to three weeks in heavy users; sleep will recover with treatment.
- Circadian anchoring: Fix rise time; morning bright light or outdoor light within 60 minutes of wake; brief, light exercise if possible.
- CBT-I core behaviors: Stimulus control (bed only for sleep; out of bed if awake more than 15 to 20 minutes; consistent wake time); gentle relaxation before bed; avoid long daytime naps (limit to 20 minutes, before 2 pm if needed).
- Sleep restriction: Calculate average total sleep time from baseline diary and set time in bed equal to total sleep time plus 30 to 45 minutes, with fixed rise time; adjust weekly based on sleep efficiency.
- Pharmacologic bridge (selective, short-term): If insomnia is severe (fewer than 3 to 4 hours sleep, pronounced wake time) and relapse risk high, consider zolpidem IR 5 to 10 mg at bedtime for up to 7 to 10 nights, or gabapentin 300 to 600 mg at dinner and 300 to 600 mg at bedtime (target 900 to 1,200 mg per day) if low misuse risk; reassess at two weeks.
Phase 2: Weeks 2 to 4 (Consolidation)
Goals: Transition off short-term sedatives, optimize CBT-I, stabilize circadian timing.
- Continue CBT-I titration: Maintain sleep restriction titration rules; expect sleep efficiency to improve (targets above 85 percent). Address maladaptive cognitions (“I’ll never sleep without weed”) via cognitive restructuring.
- Light/dark regimen: Continue daily morning bright light and evening dim light.
- Taper pharmacologic adjuncts: Zolpidem, discontinue within 7 to 10 nights or step down to alternate nights, then stop. Gabapentin, if used, reassess sleep and craving; plan taper by week 4 to 8 if stable; monitor for misuse risk.
- Consider DORA initiation: For patients with ongoing sleep onset latency or wake time despite optimized CBT-I and circadian steps, consider a DORA (for example, lemborexant 5 mg at bedtime; titrate to 10 mg if needed), acknowledging off-label status for cannabis withdrawal but strong insomnia efficacy.
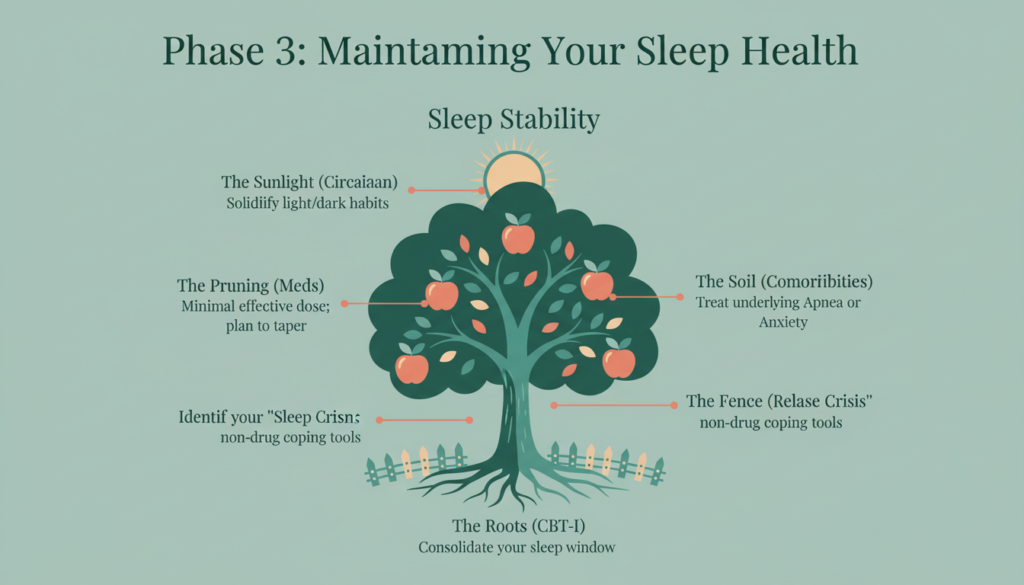
Phase 3: Weeks 5 to 12 (Maintenance and Relapse Prevention)
Goals: Durable sleep independence from cannabis; relapse prevention via sleep stability.
- Complete CBT-I course: Ensure at least four to six sessions with consolidation and cognitive work; maintain modest sleep window rather than overexpanding time in bed.
- Continue circadian hygiene: Solidify light/dark habits and fixed rise time; add weekend variability limit (no more than one hour shift).
- Pharmacologic review: If a DORA was started, plan the minimal effective dose and consider tapering after several months of stability. Avoid chronic Z-drugs or benzodiazepines in recovery.
- Address comorbidities: Screen and treat sleep apnea, depression, anxiety; treat nicotine use (nicotine replacement therapy) if co-quitting.
- Relapse planning: Identify “sleep crisis” plan, non-drug coping (relaxation scripts, out-of-bed protocol, next-day light exposure) and access to clinician support, avoiding cannabis as a fallback.
Special Considerations and Comorbidities
Co-Use of Nicotine
Nicotine withdrawal overlaps with cannabis withdrawal symptoms and time course; unaddressed nicotine cessation can amplify insomnia and relapse risk.
Consider nicotine replacement therapy during withdrawal if you are also quitting tobacco, and differentiate symptoms where possible.
Circadian Delay in Adolescents and Young Adults
Delayed sleep-wake phase disorder is common in youth and can confound insomnia. Emphasize school or work-compatible rise times, morning light, and CBT-I adapted for youth.
Avoid reliance on cannabis for sleep onset; focus on phase advances and stimulus control.
Sleep Apnea and Medical Comorbidity
A large sleep-clinic cohort found that long-term daily cannabis use was associated with greater nocturnal wakefulness, lower sleep efficiency, and more stage N1 sleep.
Cannabis users often have comorbid sleep apnea; sedatives (especially benzodiazepines) may worsen hypoventilation. Screen for apnea before initiating hypnotics; prioritize CBT-I and circadian steps, and treat apnea (for example, CPAP).
Depression and Other Psychiatric Comorbidities
Insomnia and depression are bidirectionally linked. For major depressive disorder with insomnia, treat depression per guidelines; sedating antidepressants (mirtazapine, doxepin) may be considered in selected cases but weigh metabolic effects. CBT-I improves both insomnia and PTSD symptoms and is a versatile adjunct across psychiatric comorbidity.
Measuring Progress and Adjusting Care
Use a validated sleep diary daily for at least four weeks; calculate sleep efficiency and adjust time in bed weekly per CBT-I.
Consider actigraphy to objectify wake time and sleep timing variability; this is particularly useful when subjective-objective mismatch is suspected. Reserve polysomnography for suspected sleep apnea, limb movement disorder, parasomnias, or when treatment response is atypical.
Include patient-reported outcomes (Insomnia Severity Index, daytime functioning) and relapse metrics (Timeline Followback, urine toxicology in clinical trials) to connect sleep improvements to cannabis use disorder outcomes.
Why It Matters?
Insomnia after quitting marijuana is not just uncomfortable, it is a clinically significant predictor of relapse and a barrier to sustained recovery. Understanding that withdrawal insomnia stems from neurobiological changes in CB1 receptors, REM-NREM regulation, and conditioned arousal clarifies why resuming cannabis immediately relieves symptoms but perpetuates tolerance and dependence cycles.
The durable solution is not to restore the drug state but to restore sleep health through evidence-based behavioral care and targeted treatment of comorbidities.
The most effective and durable way to sleep without weed is to build treatment around CBT-I and circadian entrainment. These are first-line, disease-modifying approaches that consolidate sleep, correct phase, and reduce long-term relapse risk.
Layer short-term pharmacotherapy selectively to bridge the withdrawal peak and reduce relapse risk, zolpidem for a few nights or gabapentin for two to four weeks in low-misuse-risk patients can meaningfully improve sleep and withdrawal severity.
For persistent insomnia beyond the acute window, consider a dual orexin receptor antagonist as the preferred pharmacologic adjunct over sedating antipsychotics or re-exposure to cannabinoids.
Sleeping without weed is achievable by combining rigorous behavioral sleep medicine with targeted, time-limited pharmacologic support. This strategy aligns with the best available evidence, minimizes new dependencies, and directly addresses the sleep-relapse link that derails so many quit attempts.
If you or someone you care about is struggling with insomnia after quitting marijuana and needs professional support to navigate withdrawal and build lasting recovery, reach out to Mosaic for compassionate, evidence-based care.